

Effects of digoxin at low serum concentrations on mortality and hospitalization in heart failure: a propensity-matched study of the DIG trial
- PMID: 17382417
- PMCID: PMC2474767
- DOI: 10.1016/j.ijcard.2006.12.001
Effects of digoxin at low serum concentrations on mortality and hospitalization in heart failure: a propensity-matched study of the DIG trial
Abstract
Background: In heart failure (HF), digoxin at low serum digoxin concentrations (SDC) reduces all-cause mortality and HF hospitalizations. However, the effects of digoxin on other cause-specific outcomes have not been studied in a propensity-matched cohort.
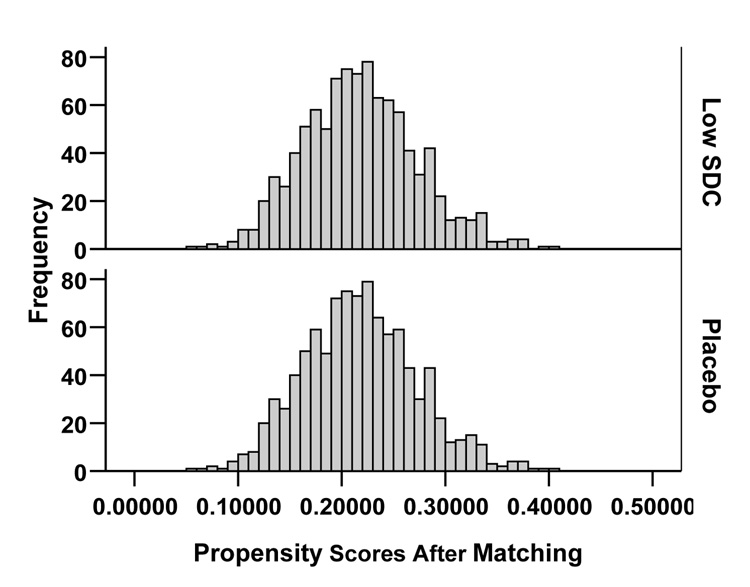
Methods: The Digitalis Investigation Group trial, conducted during 1991-1993, enrolled 7788 ambulatory chronic HF patients. This analysis focuses on 4843 patients: 982 receiving digoxin with low (0.5-0.9 ng/ml) SDC at one month, and 3861 receiving placebo and alive at one month. Propensity scores for low SDC, calculated using a non-parsimonious multivariable logistic regression model, were used to match 982 low-SDC patients with 982 placebo patients. Matched Cox regression analyses were used to determine the effect of digoxin at low SDC on outcomes.
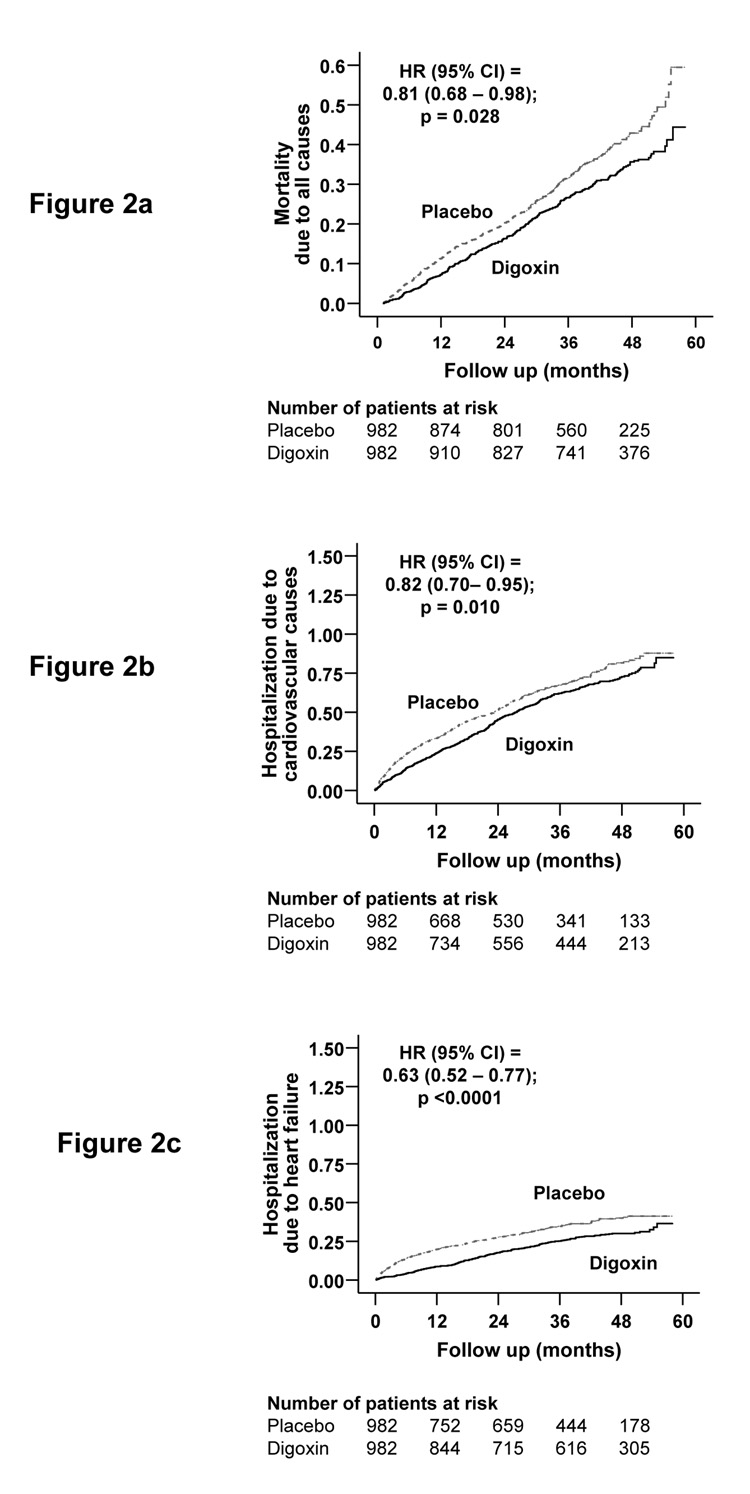
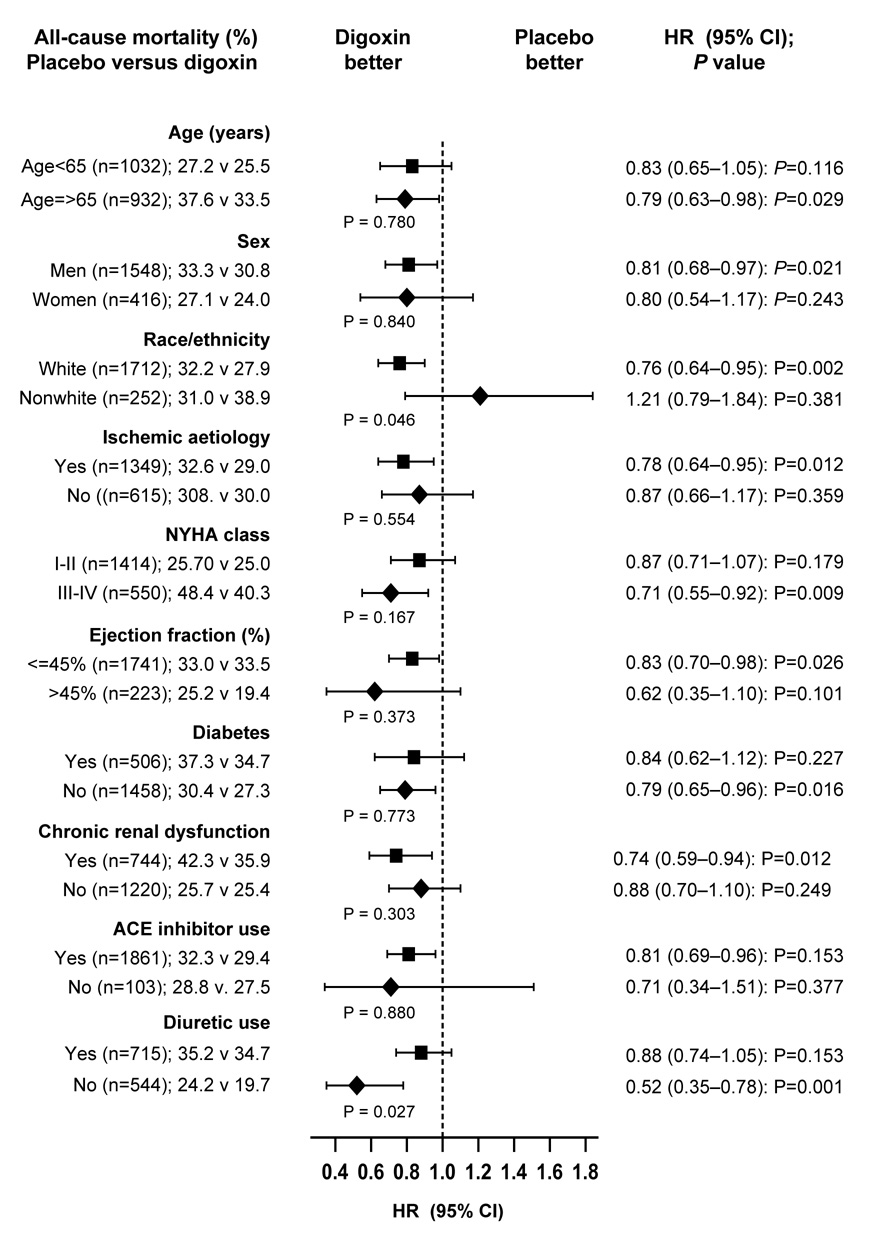
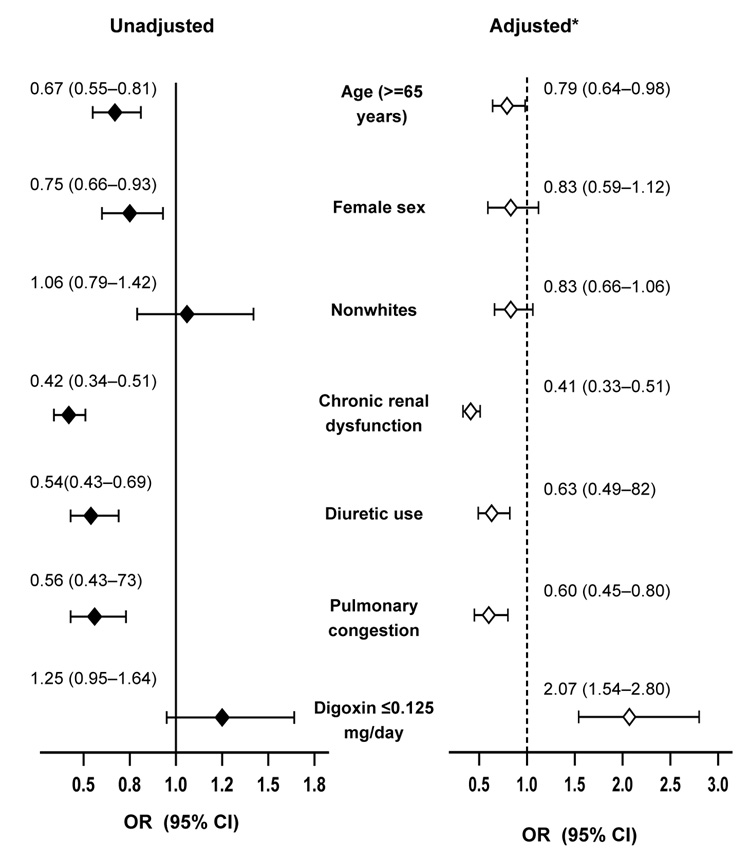
Results: All-cause mortality occurred in 315 placebo (rate, 1071/10,000 person-years) and 288 low-SDC digoxin (rate, 871/10,000 person-years) patients, respectively, during 2940 and 3305 years of follow up (hazard ratio {HR}, 0.81, 95% confidence interval {CI}, 0.68-0.98; p=0.028). Cardiovascular hospitalizations occurred in 493 placebo (2359/10,000 person-year) and 471 low-SDC digoxin (1963/10,000 person-year) patients, respectively during 2090 and 2399 years of follow up (HR, 0.82, 95% CI, 0.70-0.95; P=0.010). Low-SDC digoxin to placebo HR (95%CI) for HF mortality and HF hospitalizations were respectively, 0.65 (0.45-0.92; P=0.015) and 0.63 (0.52-0.77; P<0.0001). Low-dose digoxin (< or = 0.125 mg/day) was the strongest independent predictor of low SDC (adjusted odd ratio, 2.07, 95% CI 1.54-2.80).
Conclusions: Digoxin at low SDC significantly reduced mortality and hospitalizations in ambulatory chronic systolic and diastolic HF patients.
Figures
Comment in
-
Low-dose digoxin in heart failure.Int J Cardiol. 2009 Jul 24;136(1):90-1; author reply 91-2. doi: 10.1016/j.ijcard.2008.04.008. Epub 2008 Jul 1. Int J Cardiol. 2009. PMID: 18597868 No abstract available.
References
-
- Rahimtoola SH. Digitalis therapy for patients in clinical heart failure. Circulation. 2004;109:2942–2946. - PubMed
-
- Gheorghiade M, van Veldhuisen DJ, Colucci WS. Contemporary use of digoxin in the management of cardiovascular disorders. Circulation. 2006;113:2556–2564. - PubMed
-
- The Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336:525–533. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
