

Successful whole lung lavage in pulmonary alveolar proteinosis secondary to lysinuric protein intolerance: a case report
- PMID: 17386098
- PMCID: PMC1845139
- DOI: 10.1186/1750-1172-2-14
Successful whole lung lavage in pulmonary alveolar proteinosis secondary to lysinuric protein intolerance: a case report
Abstract
Background: Pulmonary alveolar proteinosis (PAP) is a rare disease characterised by accumulation of lipoproteinaceous material within alveoli, occurring in three clinically distinct forms: congenital, acquired and secondary. Among the latter, lysinuric protein intolerance (LPI) is a rare genetic disorder caused by defective transport of cationic amino acids. Whole Lung Lavage (WLL) is currently the gold standard therapy for severe cases of PAP.
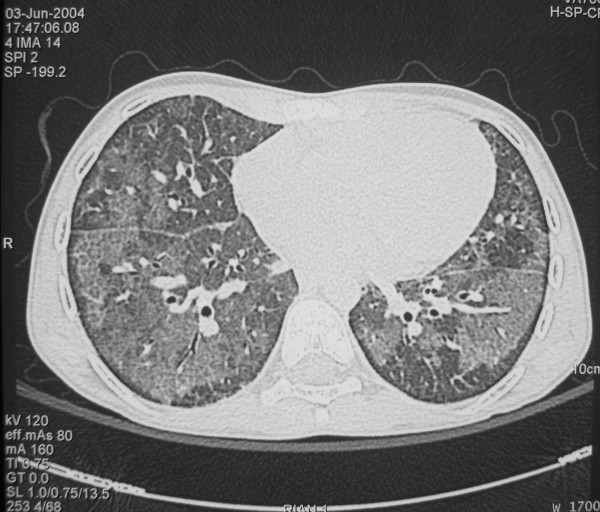
Case presentation: We describe the case of an Italian boy affected by LPI who, by the age of 10, developed digital clubbing and, by the age of 16, a mild restrictive functional impairment associated with a high-resolution computed tomography (HRCT) pattern consistent with pulmonary alveolar proteinosis. After careful assessment, he underwent WLL.
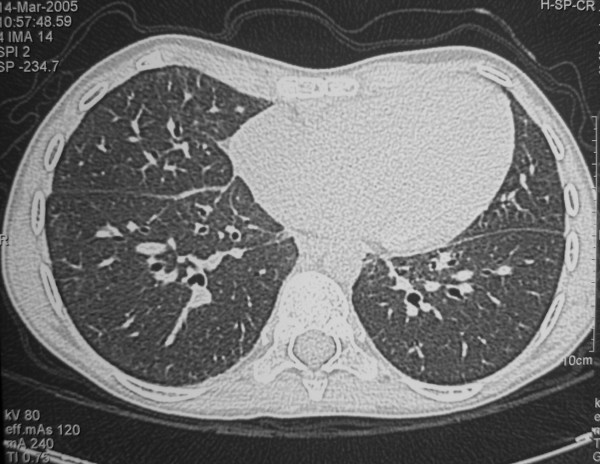
Conclusion: Two years after WLL, the patient has no clinical, radiological or functional evidence of pulmonary disease recurrence, thus suggesting that WLL may be helpful in the treatment of PAP secondary to LPI.
Figures
References
-
- Rosen SH, Castleman B, Liebow AA. Pulmonary alveolar proteinosis. N Engl J Med. 1958;258:1123–1142. - PubMed
-
- Kitamura T, Tanaka N, Watanabe J, Uchida K, Kanegasaki S, Yamada Y, Nakata K. Idiopathic pulmonary alveolar proteinosis as an autoimmune disease with neutralizing antibody against granulocyte/macrophage colony-stimulating factor. J Exp Med. 1999;190:875–880. doi: 10.1084/jem.190.6.875. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
