

A prospective study of body mass index and the risk of developing hypertension in men
- PMID: 17386342
- PMCID: PMC1920107
- DOI: 10.1016/j.amjhyper.2006.10.011
A prospective study of body mass index and the risk of developing hypertension in men
Abstract
Background: Although obesity is known to increase the risk of hypertension, few studies have prospectively evaluated body mass index (BMI) across the range of normal weight and overweight as a primary risk factor.
Methods: In this prospective cohort, we evaluated the association between BMI and risk of incident hypertension. We studied 13,563 initially healthy, nonhypertensive men who participated in the Physicians' Health Study. We calculated BMI from self-reported weight and height and defined hypertension as self-reported systolic blood pressure (BP) > or = 140 mm Hg, diastolic BP > or = 90 mm Hg, or new antihypertensive medication use.
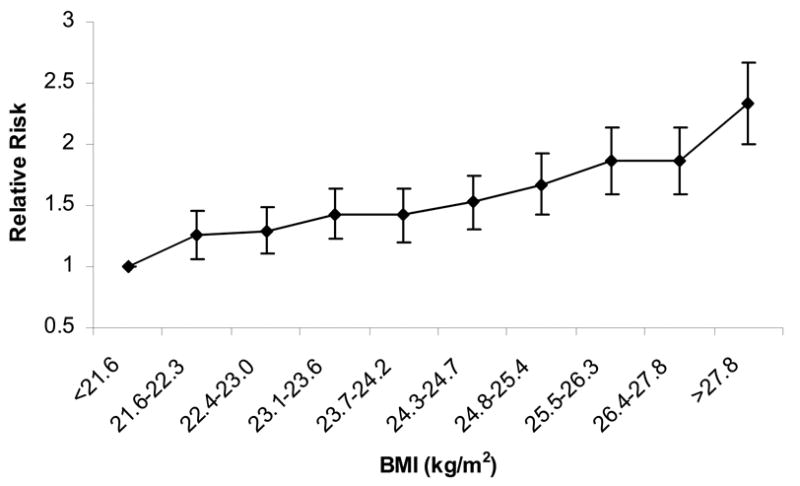
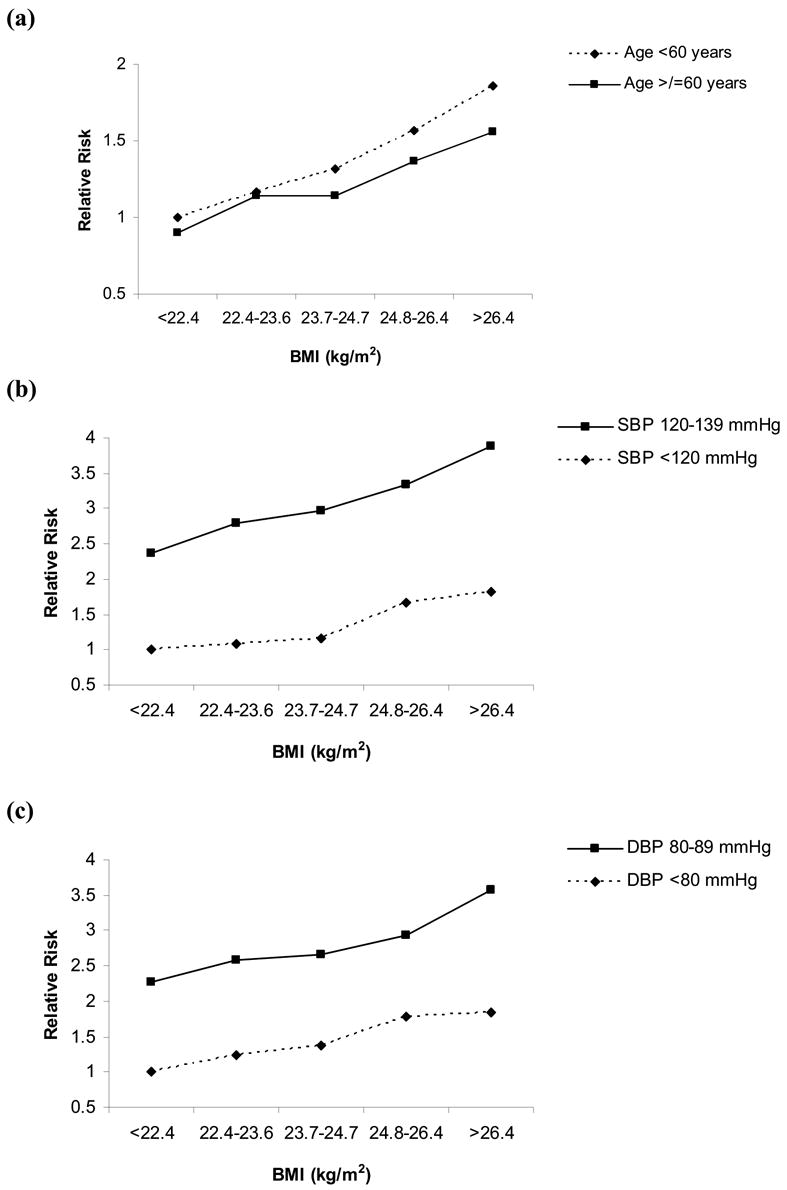
Results: After a median 14.5 years, 4920 participants developed hypertension. Higher baseline BMI, even within the "normal" range, was consistently associated with increased risk of hypertension. Compared to participants in the lowest BMI quintile (<22.4 kg/m(2)), the relative risks (95% confidence interval) of developing hypertension for men with a BMI of 22.4 to 23.6, 23.7 to 24.7, 24.8 to 26.4, and >26.4 kg/m(2) were 1.20 (1.09-1.32), 1.31 (1.19-1.44), 1.56 (1.42-1.72), and 1.85 (1.69-2.03), respectively (P for trend, <.0001). Further adjustment for diabetes, high cholesterol, and baseline BP did not substantially alter these results. We found similar associations using other BMI categories and after excluding men with smoking history, those who developed hypertension in the first 2 years, and those with diabetes, obesity, or high cholesterol at baseline.
Conclusions: In this large cohort, we found a strong gradient between higher BMI and increased risk of hypertension, even among men within the "normal" and mildly "overweight" BMI range. Approaches to reduce the risk of developing hypertension may include prevention of overweight and obesity.
Figures
Comment in
-
Body mass index as a risk factor for incident hypertension.Nat Clin Pract Endocrinol Metab. 2007 Nov;3(11):742-3. doi: 10.1038/ncpendmet0622. Epub 2007 Aug 21. Nat Clin Pract Endocrinol Metab. 2007. PMID: 17712319 No abstract available.
References
-
- Vasan RS, Beiser A, Seshadri S, Larson MG, Kannel WB, D’Agostino RB, Levy D. Residual lifetime risk for developing hypertension in middle-aged women and men: The Framingham Heart Study. JAMA. 2002;287:1003–1010. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, Jones DW, Materson BJ, Oparil S, Wright JT, Jr, Roccella EJ. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560–2572. - PubMed
-
- Stamler R, Stamler J, Gosch FC, Civinelli J, Fishman J, McKeever P, McDonald A, Dyer AR. Primary prevention of hypertension by nutritional-hygienic means. Final report of a randomized, controlled trial. JAMA. 1989;262:1801–1807. - PubMed
-
- He J, Whelton PK, Appel LJ, Charleston J, Klag MJ. Long-term effects of weight loss and dietary sodium reduction on incidence of hypertension. Hypertension. 2000;35:544–549. - PubMed
-
- Effects of weight loss and sodium reduction intervention on blood pressure and hypertension incidence in overweight people with high-normal blood pressure. The Trials of Hypertension Prevention, phase II. The Trials of Hypertension Prevention Collaborative Research Group. Arch Intern Med. 1997;157:657–667. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
