

Exquisite sensitivity of TP53 mutant and basal breast cancers to a dose-dense epirubicin-cyclophosphamide regimen
- PMID: 17388661
- PMCID: PMC1831731
- DOI: 10.1371/journal.pmed.0040090
Exquisite sensitivity of TP53 mutant and basal breast cancers to a dose-dense epirubicin-cyclophosphamide regimen
Abstract
Background: In breast cancers, only a minority of patients fully benefit from the different chemotherapy regimens currently in use. Identification of markers that could predict the response to a particular regimen would thus be critically important for patient care. In cell lines or animal models, tumor protein p53 (TP53) plays a critical role in modulating the response to genotoxic drugs. TP53 is activated in response to DNA damage and triggers either apoptosis or cell-cycle arrest, which have opposite effects on cell fate. Yet, studies linking TP53 status and chemotherapy response have so far failed to unambiguously establish this paradigm in patients. Breast cancers with a TP53 mutation were repeatedly shown to have a poor outcome, but whether this reflects poor response to treatment or greater intrinsic aggressiveness of the tumor is unknown.
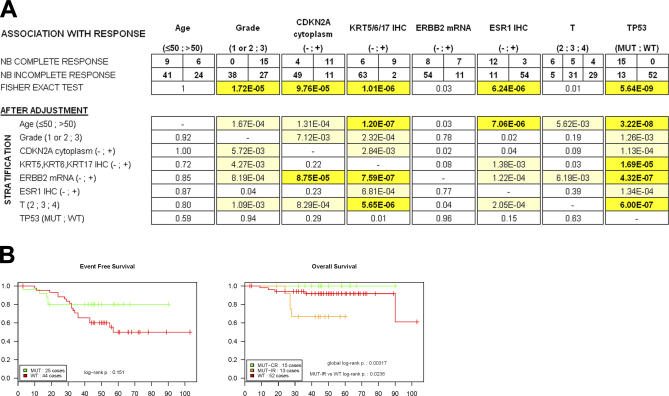
Methods and findings: In this study we analyzed 80 noninflammatory breast cancers treated by frontline (neoadjuvant) chemotherapy. Tumor diagnoses were performed on pretreatment biopsies, and the patients then received six cycles of a dose-dense regimen of 75 mg/m(2) epirubicin and 1,200 mg/m(2) cyclophosphamide, given every 14 days. After completion of chemotherapy, all patients underwent mastectomies, thus allowing for a reliable assessment of chemotherapy response. The pretreatment biopsy samples were used to determine the TP53 status through a highly efficient yeast functional assay and to perform RNA profiling. All 15 complete responses occurred among the 28 TP53-mutant tumors. Furthermore, among the TP53-mutant tumors, nine out of ten of the highly aggressive basal subtypes (defined by basal cytokeratin [KRT] immunohistochemical staining) experienced complete pathological responses, and only TP53 status and basal subtype were independent predictors of a complete response. Expression analysis identified many mutant TP53-associated genes, including CDC20, TTK, CDKN2A, and the stem cell gene PROM1, but failed to identify a transcriptional profile associated with complete responses among TP53 mutant tumors. In patients with unresponsive tumors, mutant TP53 status predicted significantly shorter overall survival. The 15 patients with responsive TP53-mutant tumors, however, had a favorable outcome, suggesting that this chemotherapy regimen can overcome the poor prognosis generally associated with mutant TP53 status.
Conclusions: This study demonstrates that, in noninflammatory breast cancers, TP53 status is a key predictive factor for response to this dose-dense epirubicin-cyclophosphamide regimen and further suggests that the basal subtype is exquisitely sensitive to this association. Given the well-established predictive value of complete responses for long-term survival and the poor prognosis of basal and TP53-mutant tumors treated with other regimens, this chemotherapy could be particularly suited for breast cancer patients with a mutant TP53, particularly those with basal features.
Conflict of interest statement
Figures


References
-
- Cardoso F, Piccart MJ. The best use of chemotherapy in the adjuvant setting. Breast. 2003;12:522–528. - PubMed
-
- Kuerer HM, Newman LA, Smith TL, Ames FC, Hunt KK, et al. Clinical course of breast cancer patients with complete pathologic primary tumor and axillary lymph node response to doxorubicin-based neoadjuvant chemotherapy. J Clin Oncol. 1999;17:460–469. - PubMed
-
- Bertheau P, Lerebours F, Mounier N, de Roquancourt A, Espie M, et al. Prognostic significance of a combined clinicopathologic score for response to primary systemic therapy in locally advanced breast cancer. Oncol Rep. 2005;14:513–520. - PubMed
-
- Kaufmann M, Hortobagyi GN, Goldhirsch A, Scholl S, Makris A, et al. Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: An update. J Clin Oncol. 2006;24:1940–1949. - PubMed
-
- Kaufmann M, von Minckwitz G, Smith R, Valero V, Gianni L, et al. International expert panel on the use of primary (preoperative) systemic treatment of operable breast cancer: Review and recommendations. J Clin Oncol. 2003;21:2600–2608. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
- Actions
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
