

Impact and process evaluation of integrated community and clinic-based HIV-1 control: a cluster-randomised trial in eastern Zimbabwe
- PMID: 17388666
- PMCID: PMC1831737
- DOI: 10.1371/journal.pmed.0040102
Impact and process evaluation of integrated community and clinic-based HIV-1 control: a cluster-randomised trial in eastern Zimbabwe
Abstract
Background: HIV-1 control in sub-Saharan Africa requires cost-effective and sustainable programmes that promote behaviour change and reduce cofactor sexually transmitted infections (STIs) at the population and individual levels.
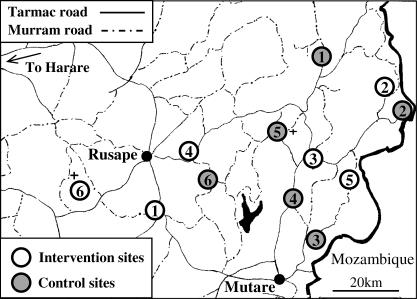
Methods and findings: We measured the feasibility of community-based peer education, free condom distribution, income-generating projects, and clinic-based STI treatment and counselling services and evaluated their impact on the incidence of HIV-1 measured over a 3-y period in a cluster-randomised controlled trial in eastern Zimbabwe. Analysis of primary outcomes was on an intention-to-treat basis. The income-generating projects proved impossible to implement in the prevailing economic climate. Despite greater programme activity and knowledge in the intervention communities, the incidence rate ratio of HIV-1 was 1.27 (95% confidence interval [CI] 0.92-1.75) compared to the control communities. No evidence was found for reduced incidence of self-reported STI symptoms or high-risk sexual behaviour in the intervention communities. Males who attended programme meetings had lower HIV-1 incidence (incidence rate ratio 0.48, 95% CI 0.24-0.98), and fewer men who attended programme meetings reported unprotected sex with casual partners (odds ratio 0.45, 95% CI 0.28-0.75). More male STI patients in the intervention communities reported cessation of symptoms (odds ratio 2.49, 95% CI 1.21-5.12).
Conclusions: Integrated peer education, condom distribution, and syndromic STI management did not reduce population-level HIV-1 incidence in a declining epidemic, despite reducing HIV-1 incidence in the immediate male target group. Our results highlight the need to assess the community-level impact of interventions that are effective amongst targeted population sub-groups.
Conflict of interest statement
Figures

References
-
- Asamoah-Odei E, Garcia Calleja JM, Boerma JT. HIV prevalence and trends in sub-Saharan Africa: No decline and large subregional differences. Lancet. 2004;364:35–40. - PubMed
-
- Anderson RM, May RM. Infectious diseases of humans: Dynamics and control. Oxford: Oxford University Press; 1991. 757
-
- Watkins SC. Navigating the AIDS epidemic in rural Malawi. Popul Dev Rev. 2005;30:673–705.
-
- UNAIDS. Trends in HIV incidence and prevalence: Natural course of the epidemic or results of behaviour change? Geneva: UNAIDS; 1999. 36
-
- Stephenson JM, Obasi A. HIV risk reduction in adolescents. Lancet. 2004;363:1177–1178. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
