

Large-scale malaria survey in Cambodia: novel insights on species distribution and risk factors
- PMID: 17389041
- PMCID: PMC1847522
- DOI: 10.1186/1475-2875-6-37
Large-scale malaria survey in Cambodia: novel insights on species distribution and risk factors
Abstract
Background: In Cambodia, estimates of the malaria burden rely on a public health information system that does not record cases occurring among remote populations, neither malaria cases treated in the private sector nor asymptomatic carriers. A global estimate of the current malaria situation and associated risk factors is, therefore, still lacking.
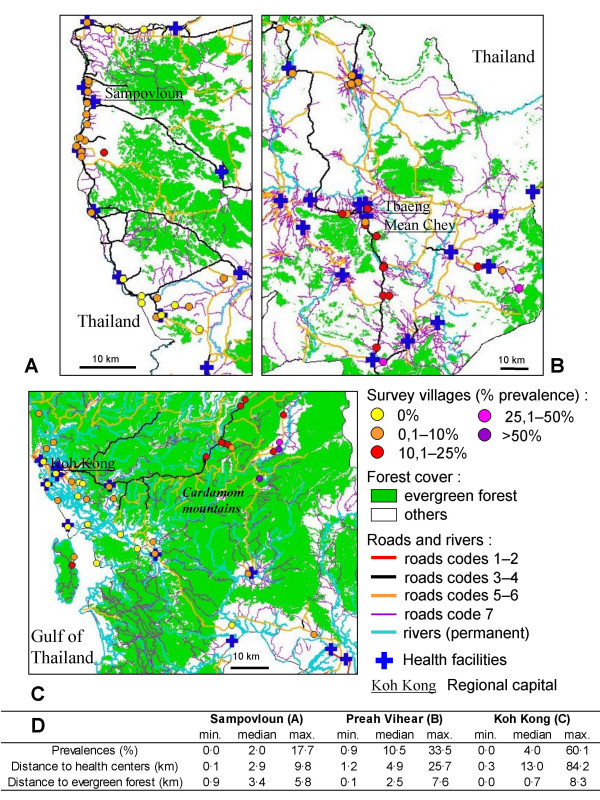
Methods: A large cross-sectional survey was carried out in three areas of multidrug resistant malaria in Cambodia, enrolling 11,652 individuals. Fever and splenomegaly were recorded. Malaria prevalence, parasite densities and spatial distribution of infection were determined to identify parasitological profiles and the associated risk factors useful for improving malaria control programmes in the country.
Results: Malaria prevalence was 3.0%, 7.0% and 12.3% in Sampovloun, Koh Kong and Preah Vihear areas. Prevalences and Plasmodium species were heterogeneously distributed, with higher Plasmodium vivax rates in areas of low transmission. Malaria-attributable fevers accounted only for 10-33% of malaria cases, and 23-33% of parasite carriers were febrile. Multivariate multilevel regression analysis identified adults and males, mostly involved in forest activities, as high risk groups in Sampovloun, with additional risks for children in forest-fringe villages in the other areas along with an increased risk with distance from health facilities.
Conclusion: These observations point to a more complex malaria situation than suspected from official reports. A large asymptomatic reservoir was observed. The rates of P. vivax infections were higher than recorded in several areas. In remote areas, malaria prevalence was high. This indicates that additional health facilities should be implemented in areas at higher risk, such as remote rural and forested parts of the country, which are not adequately served by health services. Precise malaria risk mapping all over the country is needed to assess the extensive geographical heterogeneity of malaria endemicity and risk populations, so that current malaria control measures can be reinforced accordingly.
Figures

References
-
- Olumese P. Changing the global picture of malaria – myth or reality? MIM 4th Pan-African Malaria Meeting, Yaoundé, Cameroun, 13–18 nov 2005. - PubMed
-
- World Health Organization, Regional Office for the Western Pacific: Malaria epidemiology, Cambodia http://www.wpro.who.int/sites/mvp/epidemiology/malaria/
-
- Annual Progress Reports 1999–2005. National Centre for Parasitology, Entomology and Malaria Control, Ministry of Health of Cambodia, Phnom Penh, Cambodia.
-
- Socheat D, Denis MB, Fandeur T, Zhang Z, Yang H, Xu J, Zhou X, Phompida S, Phetsouvanh R, Lwin S, Lin K, Win T, Than SW, Htut Y, Prajakwong S, Rojanawatsirivet C, Tipmontree R, Vijaykadga S, Konchom S, Cong le D, Thien NT, Thuan le K, Ringwald P, Schapira A, Christophel E, Palmer K, Arbani PR, Prasittisuk C, Rastogi R, Monti F, Urbani C, Tsuyuoka R, Hoyer S, Otega L, Thimasarn K, Songcharoen S, Meert JP, Gay F, Crissman L, Cho-Min-Naing , Chansuda W, Darasri D, Indaratna K, Singhasivanon P, Chuprapawan S, Looareesuwan S, Supavej S, Kidson C, Baimai V, Yimsamran S, Buchachart K. Mekong malaria. II. Update of malaria, multi-drug resistance and economic development in the Mekong region of Southeast Asia. Southeast Asian J Trop Med Public Health. 2003;34:1–102. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
