

Cadaveric small bowel and small bowel-liver transplantation in humans
- PMID: 1738932
- PMCID: PMC2962580
- DOI: 10.1097/00007890-199202010-00020
Cadaveric small bowel and small bowel-liver transplantation in humans
Abstract
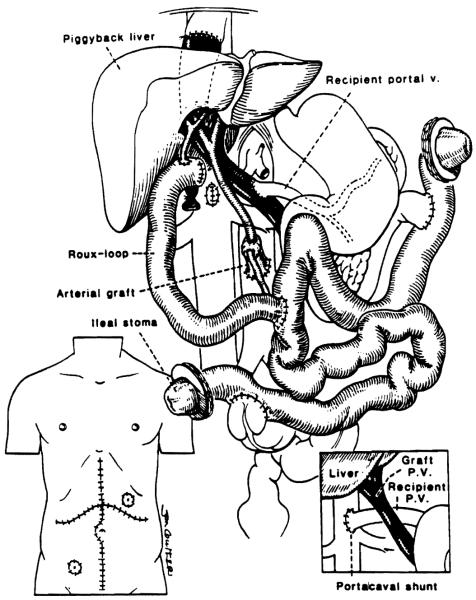
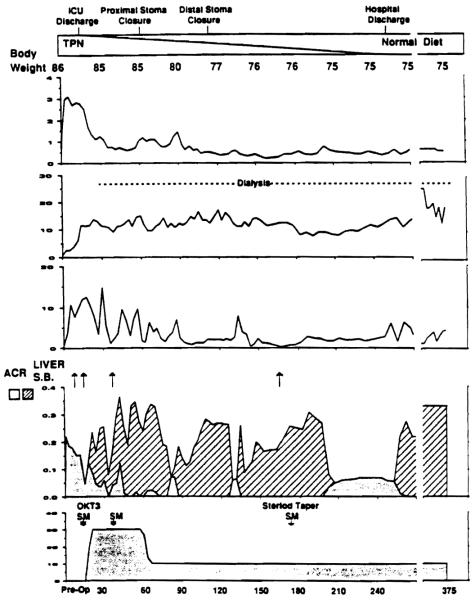
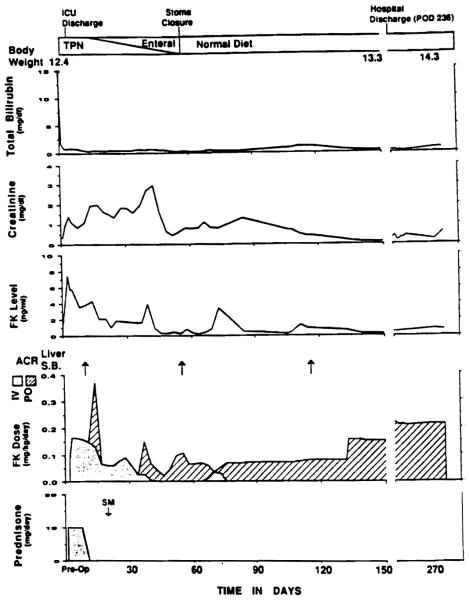
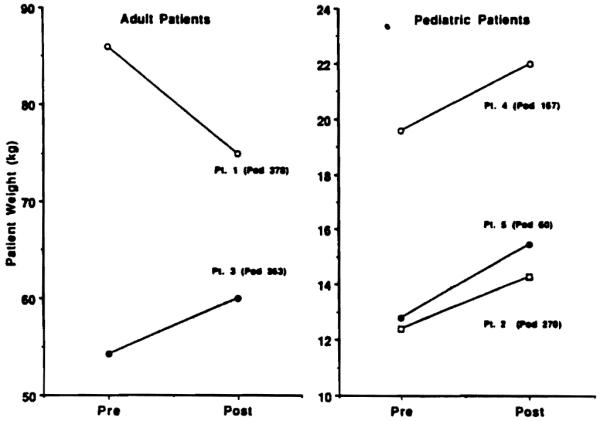
Five patients had complete cadaveric small bowel transplants under FK506 immunosuppression, one as an isolated graft and the other 4 in continuity with a liver. Three were children and two were adults. The five patients are living 2-13 months posttransplantation with complete alimentation by the intestine. The typical postoperative course was stormy, with sluggish resumption of gastrointestinal function. The patient with small intestinal transplantation alone had the most difficult course of the five, including two severe rejections, bacterial and fungal translocation with bacteremia, renal failure with the rejections, and permanent consignment to renal dialysis. The first four patients (studies on the fifth were incomplete) had replacement of the lymphoreticular cells in the graft lamina propria by their own lymphoreticular cells. Although the surgical and after-care of these patients was difficult, the eventual uniform success suggests that intestinal transplantation has moved toward becoming a practical clinical service.
Figures
References
-
- Kirkman RT. Small bowel transplantation. Transplantation. 1984;37:429. - PubMed
-
- Grant D, Wall W, Mimeault R, et al. Successful small-bowel/liver transplantation. Lancet. 1990;335:181. - PubMed
-
- Schroeder P, Goulet O, Lear PA. Small bowel transplantation: European experience [Letter] Lancet. 1990;336:110. - PubMed
-
- Goulet O, Revillon Y, Jan D, et al. Small-bowel transplantation in children. Transplant Proc. 1990;22:2499. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical