

Patient education on prostate cancer screening and involvement in decision making
- PMID: 17389534
- PMCID: PMC1838687
- DOI: 10.1370/afm.623
Patient education on prostate cancer screening and involvement in decision making
Abstract
Purpose: Many clinicians lack resources to engage patients in shared decision making for prostate cancer screening. We sought to evaluate whether previsit educational decision aids facilitate shared decision making.
Methods: This randomized controlled study compared a Web-based and a paper-based decision aid with no previsit education. Men aged 50 to 70 years undergoing a health maintenance examination at a large family practice were enrolled. The primary outcome was patient-reported level of control over the decision to be screened. Secondary outcomes included frequency of screening, patient knowledge, decisional conflict, and time spent discussing screening.
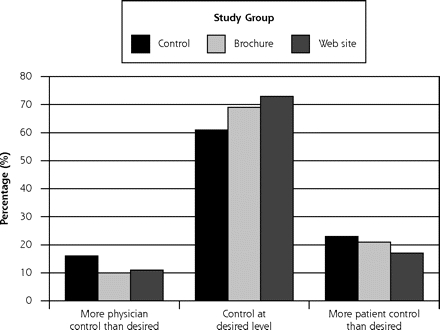
Results: A total of 497 men participated (75 control, 196 brochure, 226 Web site). Patients exposed to either aid were no more likely than control patients to report a collaborative decision: 36% of patients in each group reported equally sharing decision responsibility. Exposure to either decision aid increased patients' involvement in decision making compared with the control condition (Web site, P = .03; brochure, P = .03). Only 46% of control patients reported an active decision-making role, compared with 56% of Web site and 54% of brochure patients. Patients exposed to a decision aid answered a greater percentage of knowledge questions correctly (54% control vs 69% Web site, P <.001, and vs 69% brochure, P <.001) and were less likely to be screened (94% control vs 86% Web site, P = .06, and vs 85% brochure, P = .04).
Conclusions: Patients in the decision aid groups were more informed and more engaged in the screening decision than their control counterparts. Exposure did not promote shared decision-making control, however. Whether shared decision making is the ideal model and how to measure its occurrence are subjects for further research.
Figures


References
-
- Stamey TA, Caldwell M, McNeal JE, et al. The prostate specific antigen era in the United States is over for prostate cancer: what happened in the last 20 years? J Urol. 2004;172(4 Pt 1):1297–1301. - PubMed
-
- Thompson IM, Pauler DK, Goodman PJ, et al. Prevalence of prostate cancer among men with a prostate-specific antigen level < or = 4.0 ng per milliliter. N Engl J Med. 2004;350(22):2239–2246. - PubMed
-
- Prostate-specific antigen (PSA) best practice policy. American Urological Association (AUA). Oncology (Williston Park). 2000;14(2):267–272, 277–268, 280 passim. - PubMed
-
- Summaries for patients. Screening for prostate cancer: a recommendation from the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137(11):I48. - PubMed
-
- Smith RA, Cokkinides V, von Eschenbach AC, et al. American Cancer Society guidelines for the early detection of cancer. CA Cancer J Clin. 2002;52(1):8–22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical