

Epidemiology and outcomes of community-associated methicillin-resistant Staphylococcus aureus infection
- PMID: 17392441
- PMCID: PMC1933099
- DOI: 10.1128/JCM.02311-06
Epidemiology and outcomes of community-associated methicillin-resistant Staphylococcus aureus infection
Abstract
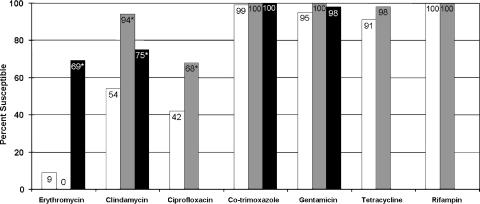
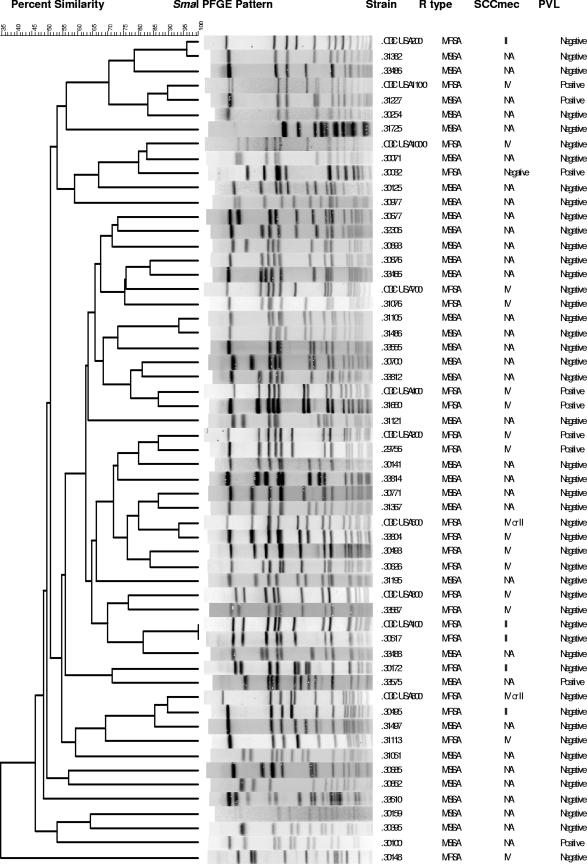
Over a 2-year period (2003 to 2005) patients with community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) and community-acquired methicillin-susceptible Staphylococcus aureus (CA-MSSA) infections were prospectively identified. Patients infected with CA-MRSA (n = 102 patients) and CA-MSSA (n = 102 patients) had median ages of 46 and 53 years, respectively; the most common sites of infection in the two groups were skin/soft tissue (80 and 93%, respectively), respiratory tract (13 and 6%, respectively), and blood (4 and 1%, respectively). Fourteen percent of patients with CA-MRSA infections and 3% of patients with CA-MSSA infections had household contacts with similar infections (P < 0.01). Among the CA-MRSA isolates, the pulsed-field gel electrophoresis (PFGE) groups detected were USA300 (49%) and USA100 (13%), with 27 PFGE groups overall; 71% of the isolates were staphylococcal chromosome cassette mec (SCCmec) type IV, 29% were SCCmec type II, and 54% had the Panton-Valentine leucocidin (PVL) gene. Among the CA-MSSA isolates there were 33 PFGE groups, with isolates of the USA200 group comprising 11%, isolates of the USA600 group comprising 11%, isolates of the USA100 group comprising 10%, and isolates of the PVL type comprising 10%. Forty-six and 18% of the patients infected with CA-MRSA and CA-MSSA, respectively, were hospitalized (P < 0.001). Fifty percent of the patients received antibiotic therapy alone, 5% received surgery alone, 30% received antibiotics and surgery, 3% received other therapy, and 12% received no treatment. The median durations of antibiotic therapy were 12 and 10 days in the CA-MRSA- and CA-MSSA-infected patients, respectively; 48 and 56% of the patients in the two groups received adequate antimicrobial therapy, respectively (P < 0.001). The clinical success rates of the initial therapy in the two groups were 61 and 84%, respectively (P < 0.001); recurrences were more common in the CA-MRSA group (recurrences were detected in 18 and 6% of the patients in the two groups, respectively [P < 0.001]). CA-MRSA was an independent predictor of clinical failure in multivariate analysis (odds ratio, 3.4; 95% confidence interval, 1.7 to 6.9). In the community setting, the molecular characteristics of the S. aureus strains were heterogeneous. CA-MRSA infections were associated with a more adverse impact on outcome than CA-MSSA infections.
Figures
References
-
- Bannerman, T. L. 2003. Staphylococcus, Micrococcus, and other catalase-positive cocci that grow aerobically, p. 384-404. In P. R. Murray, E. J. Baron, J. H. Jorgensen, M. A. Pfaller, and R. H. Yolken (ed.), Manual of clinical microbiology, 8th ed. ASM Press, Washington, DC.
-
- Centers for Disease Control and Prevention. 1999. Four pediatric deaths from community-acquired methicillin-resistant Staphylococus aureus-Minnesota and North Dakota, 1997-1999. JAMA 282:1123-1125. - PubMed
-
- Centers for Disease Control and Prevention. 2003. Methicillin-resistant Staphylococus aureus infections in correctional facilities—Georgia, California, and Texas, 2001-2003. Morb. Mortal. Wkly. Rep. 52:992-996. - PubMed
-
- Centers for Disease Control and Prevention. 2003. Methicillin-resistant Staphylococus aureus infections among competitive sports participants—Colorado, Indiana, Pennsylvania, and Los Angeles County, 2000-2003. Morb. Mortal. Wkly. Rep. 52:793-795. - PubMed
-
- Centers for Disease Control and Prevention. 2004. Community-associated methicillin-resistant Staphylococus aureus infections in Pacific Islanders—Hawaii, 2001-2003. Morb. Mortal. Wkly. Rep. 53:767-770. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
