

Effect of sleep on interictal spikes and distribution of sleep spindles on electrocorticography in children with focal epilepsy
- PMID: 17398152
- PMCID: PMC1945117
- DOI: 10.1016/j.clinph.2007.02.021
Effect of sleep on interictal spikes and distribution of sleep spindles on electrocorticography in children with focal epilepsy
Abstract
Objective: To determine how sleep with central spindles alters the spatial distribution of interictal spike frequency in children with intractable focal seizures, and whether such children have spindles arising from the medial temporal region in addition to the frontal-central region.
Methods: Seventeen children (age: 7 months-17 years) were studied using extraoperative electrocorticography (ECoG).
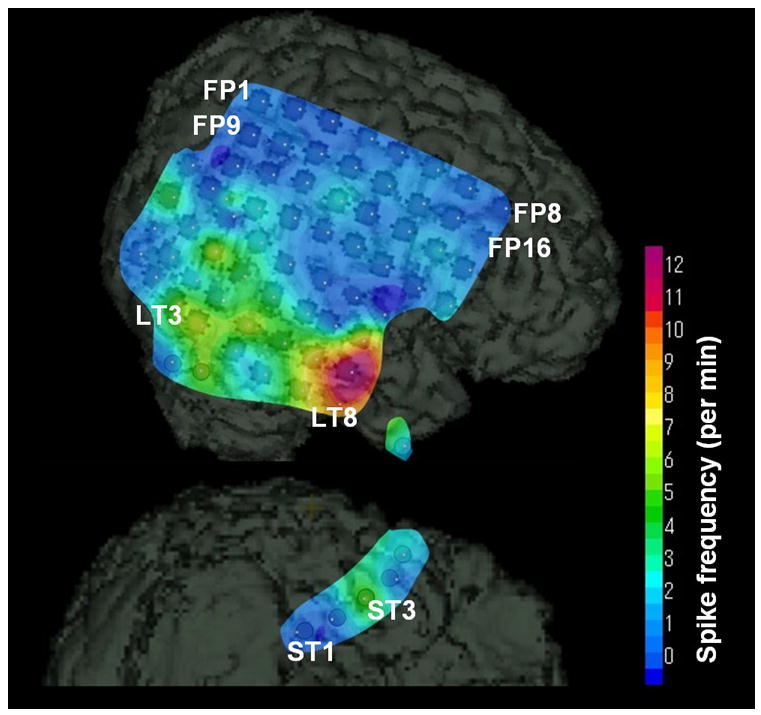
Results: Overall spike frequency across the subdural electrodes was greater during sleep with central spindles compared to wakefulness. In 13 children showing at least 1 spike/min in an electrode, the spatial distribution of spike frequency was similar during wakefulness and sleep; in addition, the spike frequency was greater in the seizure onset zones compared to the non-onset areas, regardless of wakefulness or sleep. Spindles were identified in the medial temporal region during sleep with central spindles in all 17 children.
Conclusion: Overall spike frequency may be increased by sleep with spindles, but the spatial distribution of spike frequency appears similar during wakefulness and sleep in children with intractable focal seizures.
Significance: Both awake and sleep ECoG may be useful to predict seizure onset zones in children with intractable focal epilepsy. Medial temporal spindles are present in some children with focal epilepsy.
Figures










References
-
- Asano E, Muzik O, Shah A, Juhász C, Chugani DC, Sood S, Janisse J, Ergun EL, Ahn-Ewing J, Shen C, Gotman J, Chugani HT. Quantitative interictal subdural EEG analyses in children with neocortical epilepsy. Epilepsia. 2003;44:425–434. - PubMed
-
- Brazier MA. Studies of the EEG activity of limbic structures in man. Electroencephalogr Clin Neurophysiol. 1968;25:309–318. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
