

Severity of visual field loss and health-related quality of life
- PMID: 17399676
- PMCID: PMC2731547
- DOI: 10.1016/j.ajo.2007.02.022
Severity of visual field loss and health-related quality of life
Abstract
Purpose: To examine the association between severity of visual field loss (VFL) and self-reported health-related quality of life (HRQOL) in a population-based sample.
Design: Population-based cross-sectional study.
Methods: Participants in the Los Angeles Latino Eye Study (LALES) underwent a comprehensive ophthalmic examination including visual field testing by the Humphrey Automated Field Analyzer II (Swedish Interactive Thresholding Algorithm [SITA] Standard 24-2) [Carl Zeiss Meditec, Dublin, California, USA]. Mean deviation (MD) scores were used to determine severity of VFL both as a continuous variable and stratified by severity: no VFL (MD >or= -2 decibels [dB]), mild VFL (-6 dB < MD < -2 dB), and moderate to severe VFL (MD < -6 dB). HRQOL was assessed by the Medical Outcomes Study 12-item Short-Form Health Survey (SF-12) and the National Eye Institute Visual Function Questionnaire (NEI-VFQ-25). Linear regression analyses and analysis of covariance were used to assess the relationship between HRQOL scores and VFL.
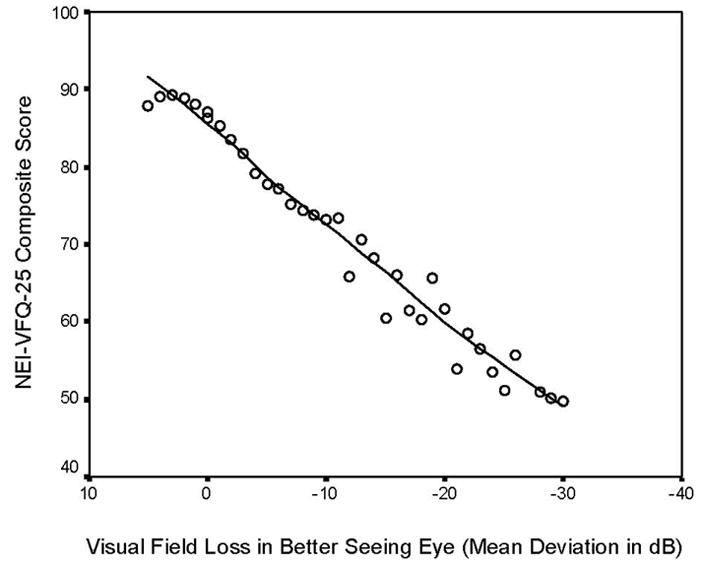
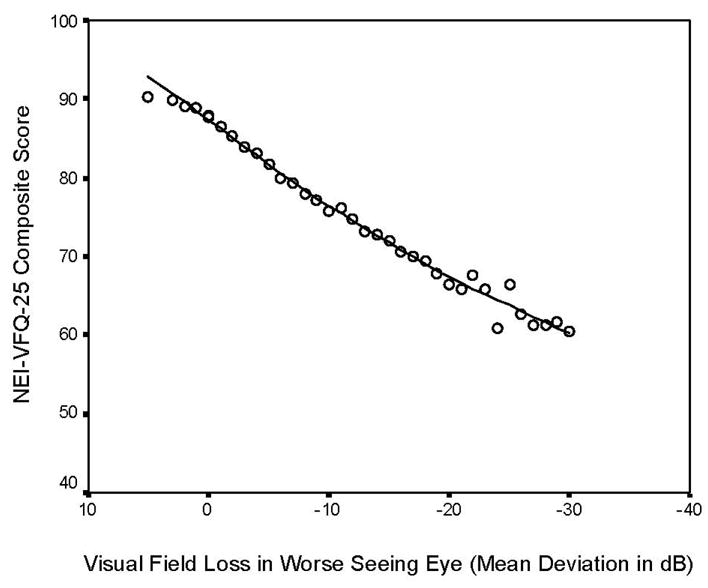
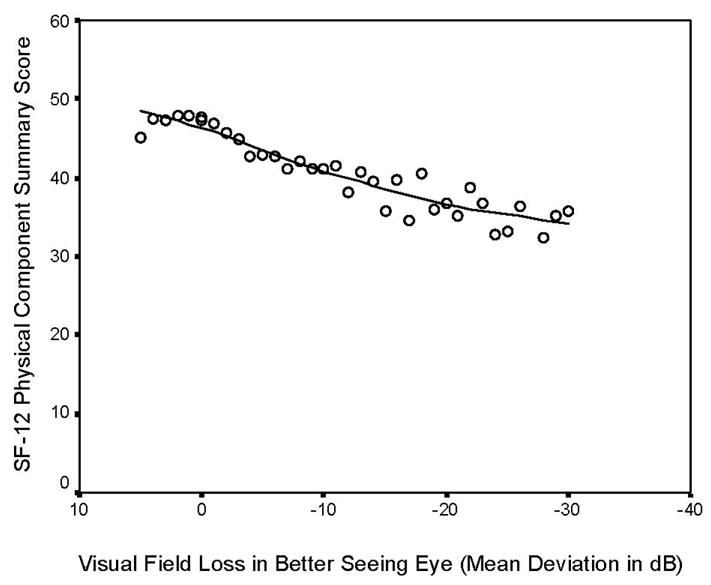
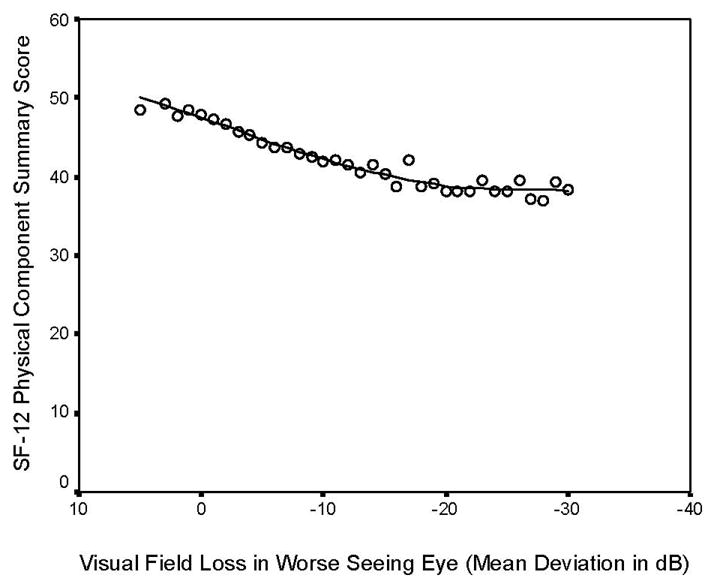
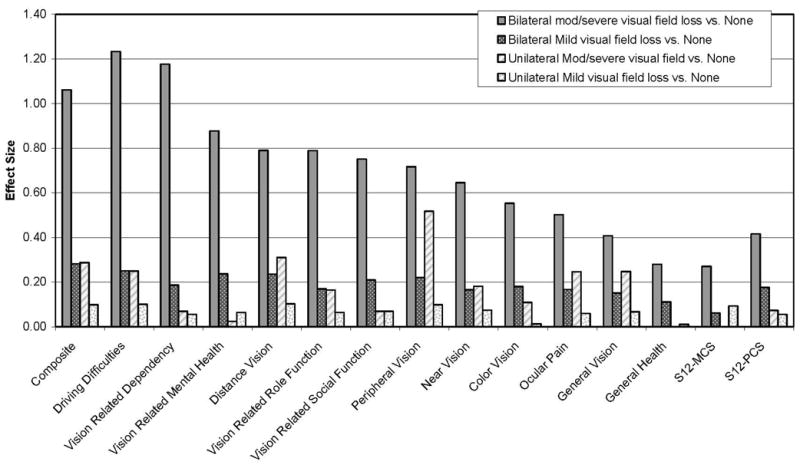
Results: Of the 5,213 participants included in this study, 18% had unilateral mild, 1.5% unilateral moderate to severe, 19% bilateral mild, and 6.5% bilateral moderate to severe VFL. Worse NEI-VFQ-25 and SF-12 HRQOL scores were associated with VFL in a linear manner. Four- to 5-dB differences in VFL were associated with a five-point difference in the NEI-VFQ-25 composite and most subscale scores. Persons with VFL had the greatest difficulty with driving activities, dependency, mental health, distance vision, and peripheral vision.
Conclusions: HRQOL is diminished even in persons with relatively mild VFL on the basis of MD scores. Prevention and management of persons with VFL may be important in preventing or reducing poor HRQOL related to difficulties in driving, distance and peripheral vision activities, and a sense of dependency.
Figures
References
-
- Friedman DS, Congdon N, Kempen J, Tielsch JM. Vision Problems in the U.S., Prevalence of Adult Vision Impairment and Age-Related Eye Disease in America. Bethesda, MD: National Eye Institute; 2002. p. 1.
-
- Sherwood MB, Garcia-Siekavizza A, Meltzer MI, Hebert A, Burns AF, McGorray S. Glaucoma’s impact on quality of life and its relation to clinical indicators. A pilot study Ophthalmology. 1998;105:561–6. - PubMed
-
- Klein BE, Klein R, Lee KE, Cruickshanks KJ. Performance-based and self-assessed measures of visual function as related to history of falls, hip fractures, and measured gait time. The Beaver Dam Eye Study. Ophthalmology. 1998;105:160–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
