

Confidential reporting of patient safety events in primary care: results from a multilevel classification of cognitive and system factors
- PMID: 17403753
- PMCID: PMC2653163
- DOI: 10.1136/qshc.2006.020909
Confidential reporting of patient safety events in primary care: results from a multilevel classification of cognitive and system factors
Abstract
Objective: To classify events of actual or potential harm to primary care patients using a multilevel taxonomy of cognitive and system factors.
Methods: Observational study of patient safety events obtained via a confidential but not anonymous reporting system. Reports were followed up with interviews where necessary. Events were analysed for their causes and contributing factors using causal trees and were classified using the taxonomy. Five general medical practices in the West Midlands were selected to represent a range of sizes and types of patient population. All practice staff were invited to report patient safety events. Main outcome measures were frequencies of clinical types of events reported, cognitive types of error, types of detection and contributing factors; and relationship between types of error, practice size, patient consequences and detection.
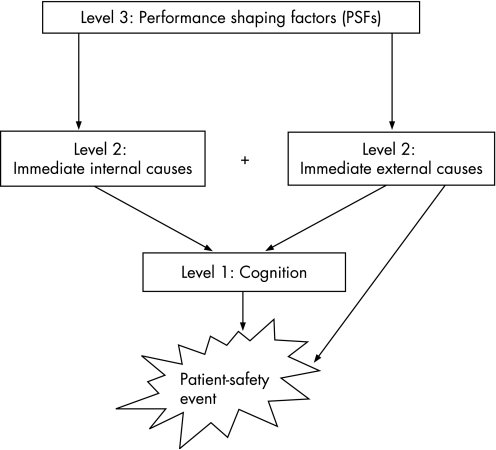
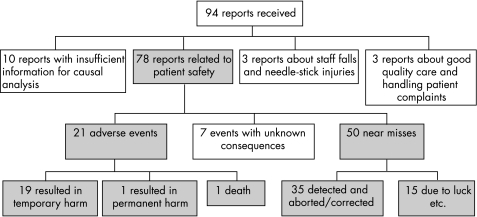
Results: 78 reports were relevant to patient safety and analysable. They included 21 (27%) adverse events and 50 (64%) near misses. 16.7% (13/71) had serious patient consequences, including one death. 75.7% (59/78) had the potential for serious patient harm. Most reports referred to administrative errors (25.6%, 20/78). 60% (47/78) of the reports contained sufficient information to characterise cognition: "situation assessment and response selection" was involved in 45% (21/47) of these reports and was often linked to serious potential consequences. The most frequent contributing factor was work organisation, identified in 71 events. This included excessive task demands (47%, 37/71) and fragmentation (28%, 22/71).
Conclusions: Even though most reported events were near misses, events with serious patient consequences were also reported. Failures in situation assessment and response selection, a cognitive activity that occurs in both clinical and administrative tasks, was related to serious potential harm.
Conflict of interest statement
Competing interests: None.
References
-
- Sandars J, Esmail A. The frequency and nature of error in primary care: understanding the diversity across studies. Fam Pract 200320231–236. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources