

An integrated care pathway for menorrhagia across the primary-secondary interface: patients' experience, clinical outcomes, and service utilisation
- PMID: 17403756
- PMCID: PMC2653147
- DOI: 10.1136/qshc.2005.016782
An integrated care pathway for menorrhagia across the primary-secondary interface: patients' experience, clinical outcomes, and service utilisation
Abstract
Background: "Referral" characterises a significant area of interaction between primary and secondary care. Despite advantages, it can be inflexible, and may lead to duplication.
Objective: To examine the outcomes of an integrated model that lends weight to general practitioner (GP)-led evidence based care.
Design: A prospective, non-random comparison of two services: women attending the new (Bridges) pathway compared with those attending a consultant-led one-stop menstrual clinic (OSMC). Patients' views were examined using patient career diaries, health and clinical outcomes, and resource utilisation. Follow-up was for 8 months.
Setting: A large teaching hospital and general practices within one primary care trust (PCT).
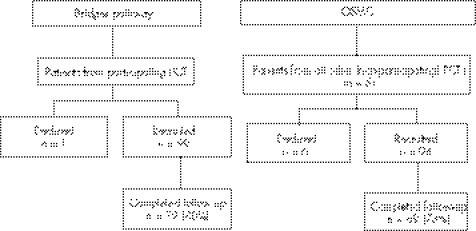
Results: Between March 2002 and June 2004, 99 women in the Bridges pathway were compared with 94 women referred to the OSMC by GPs from non-participating PCTs. The patient career diary demonstrated a significant improvement in the Bridges group for patient information, fitting in at the point of arrangements made for the patient to attend hospital (ease of access) (p<0.001), choice of doctor (p = 0.020), waiting time for an appointment (p<0.001), and less "limbo" (patient experience of non-coordination between primary and secondary care) (p<0.001). At 8 months there were no significant differences between the two groups in surgical and medical treatment rates or in the use of GP clinic appointments. Significantly fewer (traditional) hospital outpatient appointments were made in the Bridges group than in the OSMC group (p<0.001).
Conclusion: A general practice-led model of integrated care can significantly reduce outpatient attendance while improving patient experience, and maintaining the quality of care.
Conflict of interest statement
Conflicts of interest: None.
Similar articles
-
Child Health General Practice Hubs: a service evaluation.Arch Dis Child. 2016 Apr;101(4):333-7. doi: 10.1136/archdischild-2015-308910. Epub 2015 Dec 23. Arch Dis Child. 2016. PMID: 26699536
-
Feasibility and acceptability of providing nurse counsellor genetics clinics in primary care.J Adv Nurs. 2006 Mar;53(5):591-604. doi: 10.1111/j.1365-2648.2006.03760.x. J Adv Nurs. 2006. PMID: 16499680
-
The use and overlap of AED and general practice services by patients registered at two inner London general practices.Br J Gen Pract. 1998 Sep;48(434):1575-9. Br J Gen Pract. 1998. PMID: 9830182 Free PMC article.
-
Systematic review of the effectiveness, barriers and facilitators to general practitioner engagement with specialist secondary services in integrated palliative care.BMJ Support Palliat Care. 2018 Dec;8(4):385-399. doi: 10.1136/bmjspcare-2016-001125. Epub 2017 Feb 14. BMJ Support Palliat Care. 2018. PMID: 28196828
-
'We offer hope to people'.Nurs Times. 2003 Feb 11-17;99(6):38-9. Nurs Times. 2003. PMID: 12621894 Review. No abstract available.
Cited by
-
Interventions to improve access to care for abnormal uterine bleeding: A systematic scoping review.Int J Gynaecol Obstet. 2023 Jan;160(1):38-48. doi: 10.1002/ijgo.14224. Epub 2022 May 5. Int J Gynaecol Obstet. 2023. PMID: 35429335 Free PMC article.
-
Referral interventions from primary to specialist care: a systematic review of international evidence.Br J Gen Pract. 2014 Dec;64(629):e765-74. doi: 10.3399/bjgp14X682837. Br J Gen Pract. 2014. PMID: 25452541 Free PMC article.
-
Open-access transvaginal sonography in women of reproductive age with abnormal vaginal bleeding: a descriptive study in general practice.Br J Gen Pract. 2011 Jun;61(587):e340-6. doi: 10.3399/bjgp11X578016. Br J Gen Pract. 2011. PMID: 21801513 Free PMC article.
-
Can guidelines improve referral to elective surgical specialties for adults? A systematic review.Qual Saf Health Care. 2010 Jun;19(3):187-94. doi: 10.1136/qshc.2008.029918. Epub 2010 Mar 8. Qual Saf Health Care. 2010. PMID: 20211956 Free PMC article.
-
Endometrial sampling in low-risk patients with abnormal uterine bleeding: a systematic review and meta-synthesis.BMC Fam Pract. 2018 Jul 30;19(1):135. doi: 10.1186/s12875-018-0817-3. BMC Fam Pract. 2018. PMID: 30060741 Free PMC article.
References
-
- Waghorn A, McKee M, Thompson J. Surgical outpatients: challenges and responses. Br J Surg 199784300–307. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources