

Psychosocial treatments for bipolar depression: a 1-year randomized trial from the Systematic Treatment Enhancement Program
- PMID: 17404119
- PMCID: PMC3579612
- DOI: 10.1001/archpsyc.64.4.419
Psychosocial treatments for bipolar depression: a 1-year randomized trial from the Systematic Treatment Enhancement Program
Abstract
Context: Psychosocial interventions have been shown to enhance pharmacotherapy outcomes in bipolar disorder.
Objective: To examine the benefits of 4 disorder-specific psychotherapies in conjunction with pharmacotherapy on time to recovery and the likelihood of remaining well after an episode of bipolar depression.
Design: Randomized controlled trial.
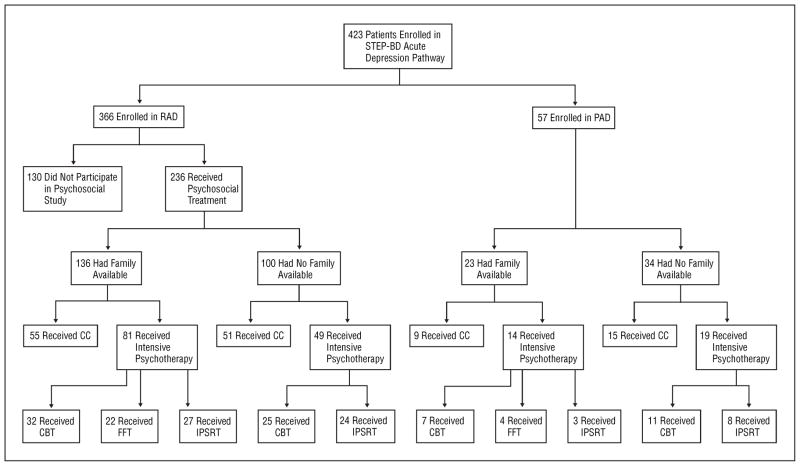
Setting: Fifteen clinics affiliated with the Systematic Treatment Enhancement Program for Bipolar Disorder. Patients A total of 293 referred outpatients with bipolar I or II disorder and depression treated with protocol pharmacotherapy were randomly assigned to intensive psychotherapy (n = 163) or collaborative care (n = 130), a brief psychoeducational intervention.
Interventions: Intensive psychotherapy was given weekly and biweekly for up to 30 sessions in 9 months according to protocols for family-focused therapy, interpersonal and social rhythm therapy, and cognitive behavior therapy. Collaborative care consisted of 3 sessions in 6 weeks.
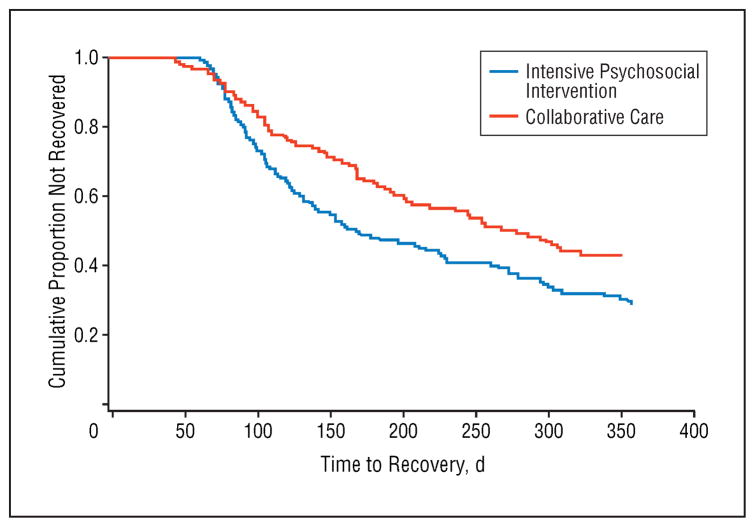
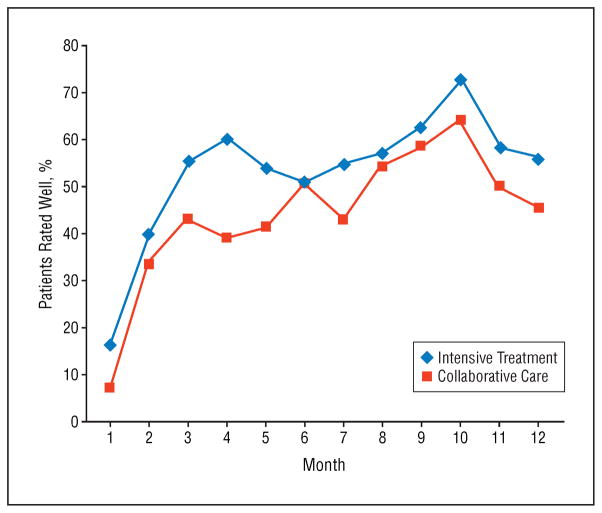
Main outcome measures: Outcome assessments were performed by psychiatrists at each pharmacotherapy visit. Primary outcomes included time to recovery and the proportion of patients classified as well during each of 12 study months.
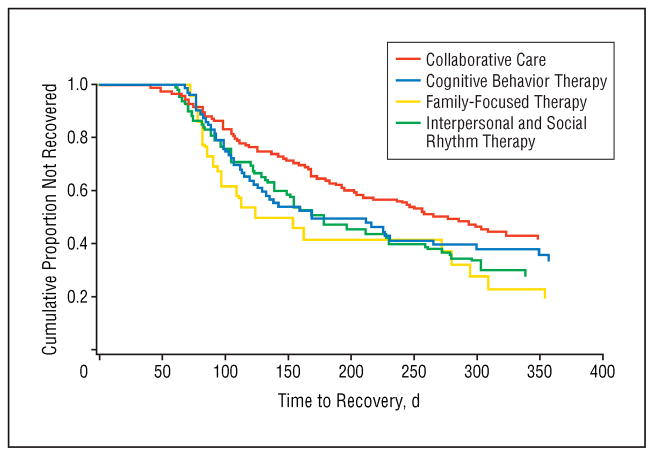
Results: All analyses were by intention to treat. Rates of attrition did not differ across the intensive psychotherapy (35.6%) and collaborative care (30.8%) conditions. Patients receiving intensive psychotherapy had significantly higher year-end recovery rates (64.4% vs 51.5%) and shorter times to recovery than patients in collaborative care (hazard ratio, 1.47; 95% confidence interval, 1.08-2.00; P = .01). Patients in intensive psychotherapy were 1.58 times (95% confidence interval, 1.17-2.13) more likely to be clinically well during any study month than those in collaborative care (P = .003). No statistically significant differences were observed in the outcomes of the 3 intensive psychotherapies.
Conclusions: Intensive psychosocial treatment as an adjunct to pharmacotherapy was more beneficial than brief treatment in enhancing stabilization from bipolar depression. Future studies should compare the cost-effectiveness of models of psychotherapy for bipolar disorder.
Trial registration: clinicaltrials.gov Identifier: NCT00012558.
Figures
Comment in
-
Is psychosocial management effective?Arch Gen Psychiatry. 2007 Dec;64(12):1451; author reply 1452-3. doi: 10.1001/archpsyc.64.12.1451-b. Arch Gen Psychiatry. 2007. PMID: 18056554 No abstract available.
References
-
- Gitlin MJ, Swendsen J, Heller TL, Hammen C. Relapse and impairment in bipolar disorder. Am J Psychiatry. 1995;152:1635–1640. - PubMed
-
- Coryell W, Scheftner W, Keller M, Endicott J, Maser J, Klerman GL. The enduring psychosocial consequences of mania and depression. Am J Psychiatry. 1993;150:720–727. - PubMed
-
- Judd LL, Akiskal HS, Schettler PJ, Coryell W, Endicott J, Maser JD, Solomon DA, Leon AC, Keller MB. A prospective investigation of the natural history of the long-term weekly symptomatic status of bipolar II disorder. Arch Gen Psychiatry. 2003;60:261–269. - PubMed
-
- Judd LL, Akiskal HS, Schettler PJ, Endicott J, Maser J, Solomon DA, Leon AC, Rice JA, Keller MB. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry. 2002;59:530–537. - PubMed
-
- Calabrese JR, Hirschfeld RM, Frye MA, Reed ML. Impact of depressive symptoms compared with manic symptoms in bipolar disorder: results of a U.S. community-based sample. J Clin Psychiatry. 2004;65:1499–1504. - PubMed
