

Cardiac structure and ventricular-vascular function in persons with heart failure and preserved ejection fraction from Olmsted County, Minnesota
- PMID: 17404159
- PMCID: PMC2001291
- DOI: 10.1161/CIRCULATIONAHA.106.659763
Cardiac structure and ventricular-vascular function in persons with heart failure and preserved ejection fraction from Olmsted County, Minnesota
Erratum in
- Circulation. 2007 May 22;115(20):e535
Abstract
Background: Mechanisms purported to contribute to the pathophysiology of heart failure with normal ejection fraction (HFnlEF) include diastolic dysfunction, vascular and left ventricular systolic stiffening, and volume expansion. We characterized left ventricular volume, effective arterial elastance, left ventricular end-systolic elastance, and left ventricular diastolic elastance and relaxation noninvasively in consecutive HFnlEF patients and appropriate controls in the community.
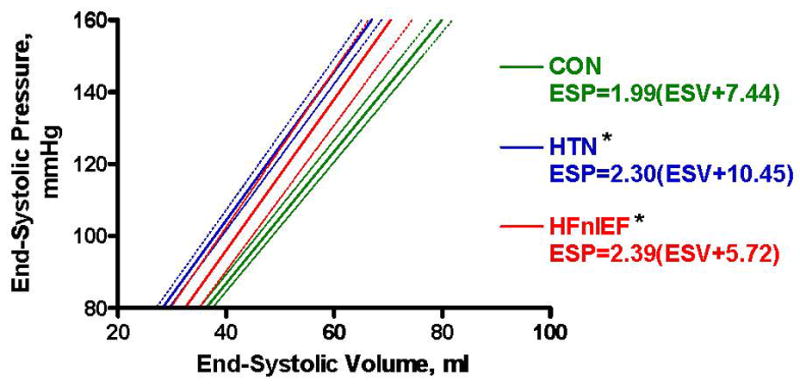
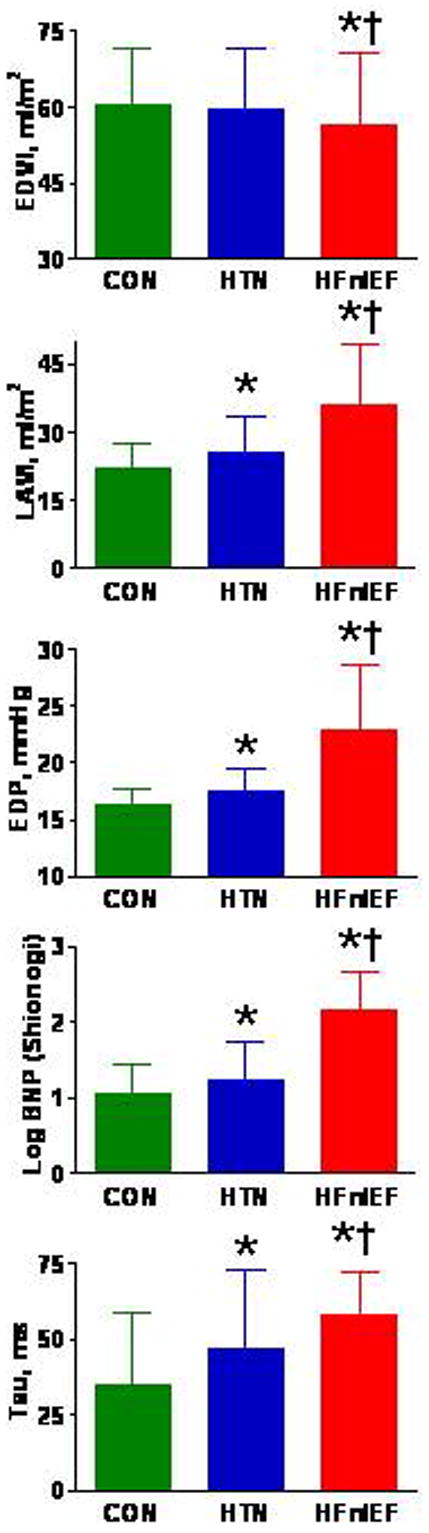
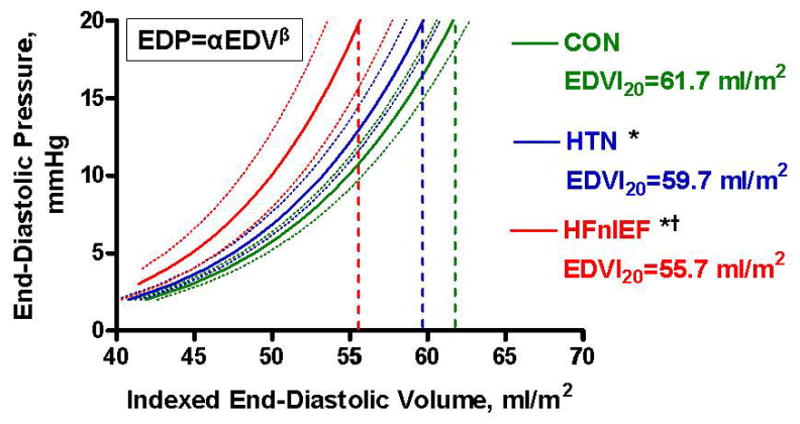
Methods and results: Olmsted County (Minn) residents without cardiovascular disease (n=617), with hypertension but no heart failure (n=719), or with HFnlEF (n=244) were prospectively enrolled. End-diastolic volume index was determined by echo Doppler. End-systolic elastance was determined using blood pressure, stroke volume, ejection fraction, timing intervals, and estimated normalized ventricular elastance at end diastole. Tissue Doppler e' velocity was used to estimate the time constant of relaxation. End-diastolic volume (EDV) and Doppler-derived end-diastolic pressure (EDP) were used to derive the diastolic curve fitting (alpha) and stiffness (beta) constants (EDP=alphaEDVbeta). Comparisons were adjusted for age, sex, and body size. HFnlEF patients had more severe renal dysfunction, yet smaller end-diastolic volume index and cardiac output and increased EDP compared with both hypertensive and healthy controls. Arterial elastance and ventricular end-systolic elastance were similarly increased in hypertensive controls and HFnlEF patients compared with healthy controls. In contrast, HFnlEF patients had more impaired relaxation and increased diastolic stiffness compared with either control group.
Conclusions: From these cross-sectional observations, we speculate that the progression of diastolic dysfunction plays a key role in the development of heart failure symptoms in persons with hypertensive heart disease.
Conflict of interest statement
Conflict of interest disclosures
None.
Figures
Comment in
-
Letter by Tartiere et al regarding article, "Cardiac structure and ventricular-vascular function in persons with heart failure and preserved ejection fraction from Olmsted County, Minnesota".Circulation. 2007 Dec 11;116(24):e562; author reply e563. doi: 10.1161/CIRCULATIONAHA.107.714394. Circulation. 2007. PMID: 18071083 No abstract available.
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–9. - PubMed
-
- Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure--abnormalities in active relaxation and passive stiffness of the left ventricle. N Engl J Med. 2004;350:1953–9. - PubMed
-
- Maurer MS, King DL, El-Khoury Rumbarger L, Packer M, Burkhoff D. Left heart failure with a normal ejection fraction: identification of different pathophysiologic mechanisms. J Card Fail. 2005;11:177–87. - PubMed
-
- Kawaguchi M, Hay I, Fetics B, Kass DA. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: implications for systolic and diastolic reserve limitations. Circulation. 2003;107:714–20. - PubMed
-
- Baicu CF, Zile MR, Aurigemma GP, Gaasch WH. Left ventricular systolic performance, function, and contractility in patients with diastolic heart failure. Circulation. 2005;111:2306–12. - PubMed
