

Systematic review, including meta-analyses, on the management of locally advanced pancreatic cancer using radiation/combined modality therapy
- PMID: 17406358
- PMCID: PMC2360143
- DOI: 10.1038/sj.bjc.6603719
Systematic review, including meta-analyses, on the management of locally advanced pancreatic cancer using radiation/combined modality therapy
Abstract
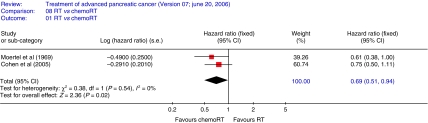
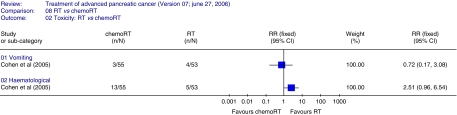
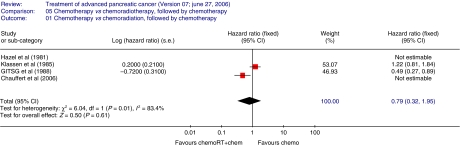
There is no consensus on the management of locally advanced pancreatic cancer, with either chemotherapy or combined modality approaches being employed (Maheshwari and Moser, 2005). No published meta-analysis (Fung et al, 2003; Banu et al, 2005; Liang, 2005; Bria et al, 2006; Milella et al, 2006) has included randomised controlled trials employing radiation therapy. The aim of this systematic review was to compare the following: (i) chemoradiation followed by chemotherapy (combined modality therapy) vs best supportive care (ii) radiotherapy vs chemoradiation (iii) radiotherapy vs combined modality therapy (iv) chemotherapy vs combined modality therapy (v) 5FU-based combined modality treatment vs another-agent-based combined modality therapy. Relevant randomised controlled trials were identified by searching databases, trial registers and conference proceedings. The primary end point was overall survival and secondary end points were progression-free survival/time-to-progression, response rate and adverse events. Survival data were summarised using hazard ratio (HR) and response-rate/adverse-event data with relative risk. Eleven trials involving 794 patients met the inclusion criteria. Length of survival with chemoradiation was increased compared with radiotherapy alone (two trials, 168 patients, HR 0.69; 95% confidence interval (CI) 0.51-0.94), but chemoradiation followed by chemotherapy did not lead to a survival advantage over chemotherapy alone (two trials, 134 patients, HR 0.79; CI 0.32-1.95). Meta-analyses could not be performed for the other comparisons. A survival benefit was demonstrated for chemoradiation over radiotherapy alone. Chemoradiation followed by chemotherapy did not demonstrate any survival advantage over chemotherapy alone, but important clinical differences cannot be ruled out due to the wide CI.
Figures
References
-
- American Cancer Society (2003) Cancer Facts and Figures 2003. American Cancer Society: Atlanta
-
- Banu E, Oudard S, Banu A, Fodor A, Landi B, Lecomte T, Laurent-Puig P, Cugnenc PJ, Andrieu JM (2005) Cumulative meta-analysis of randomised trials comparing gemcitabine-based chemotherapy vs gemcitabine alone in patients with advanced or metastatic pancreatic cancer. In ASCO Annual Meeting, abstract no. 4101, Orlando, USA
-
- Bria E, Carlini P, Gelibter A, Ruggeri E, Ceribelli A, Pino M, Terzoli E, Cognetti F, Giannarelli D, Milella M (2006) Current status of targeted agents in advanced pancreatic cancer (APC): A pooled analysis of 2,361 patients (pts) enrolled in six phase III trials. J Clin Oncol 24: 4126
-
- Cardenes H, Chiorean E, DeWitt J, Schmidt M, Loehrer P (2006) Locally advanced pancreatic cancer: Current therapeutic approach. Oncologist 11: 612–623 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
