Application of a microstructural constitutive model of the pulmonary artery to patient-specific studies: validation and effect of orthotropy
- PMID: 17408324
- PMCID: PMC3114451
- DOI: 10.1115/1.2485780
Application of a microstructural constitutive model of the pulmonary artery to patient-specific studies: validation and effect of orthotropy
Abstract
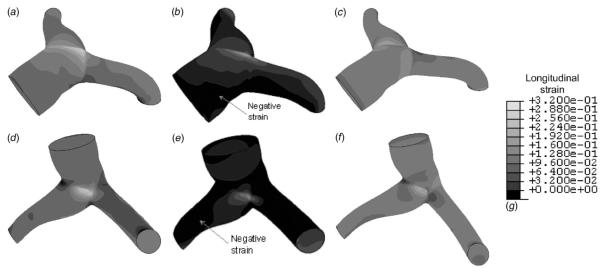
We applied a statistical mechanics based microstructural model of pulmonary artery mechanics, developed from our previous studies of rats with pulmonary arterial hypertension (PAH), to patient-specific clinical studies of children with PAH. Our previous animal studies provoked the hypothesis that increased cross-linking density of the molecular chains may be one biological remodeling mechanism by which the PA stiffens in PAH. This study appears to further confirm this hypothesis since varying molecular cross-linking density in the model allows us to simulate the changes in the P-D loops between normotensive and hypertensive conditions reasonably well. The model was combined with patient-specific three-dimensional vascular anatomy to obtain detailed information on the topography of stresses and strains within the proximal branches of the pulmonary vasculature. The effect of orthotropy on stressstrain within the main and branch PAs obtained from a patient was explored. This initial study also puts forward important questions that need to be considered before combining the microstructural model with complex patient-specific vascular geometries.
Figures









References
-
- Anthony G, Durmowicz MD, Stenmark KR. Mechanisms of Structural Remodeling in Chronic Pulmonary Hypertension. Pediatr. Rev. 1999;20:e91–e102. - PubMed
-
- Lanning C, Chen SY, Hangsen A, Chang D, Chan KC, Shandas R. Dynamic Three-dimensional Reconstruction and Modeling of Cardiovascular Anatomy in Children With Congenital Heart Disease Using Biplane Angiography. Biomed. Sci. 2004;40:200–205. - PubMed
-
- DeGroff CG, Birnbaum B, Shandas R, Orlando W, Hertzberg JR. Computational Simulations of the Total Cavo-Pulmonary Connection: Insights Into Optimizing Numerical Solutions. Pediatr. Cardiol. 2005;27:135–146. - PubMed
-
- Reuben SR. Compliance of the Human Pulmonary Arterial System in Disease. Circ. Res. 1971;29:40–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources