

The spine in Paget's disease
- PMID: 17410356
- PMCID: PMC1934928
- DOI: 10.1007/s00256-006-0270-6
The spine in Paget's disease
Abstract
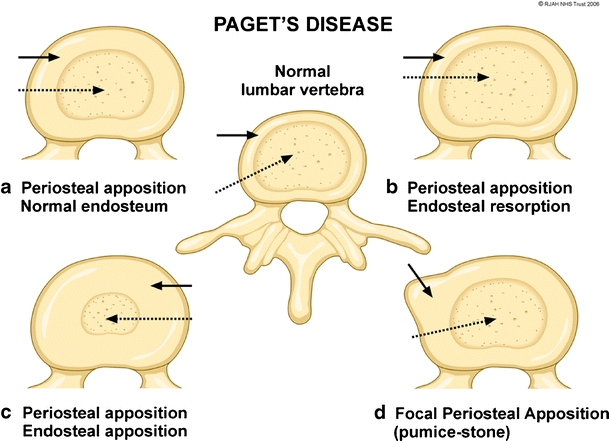
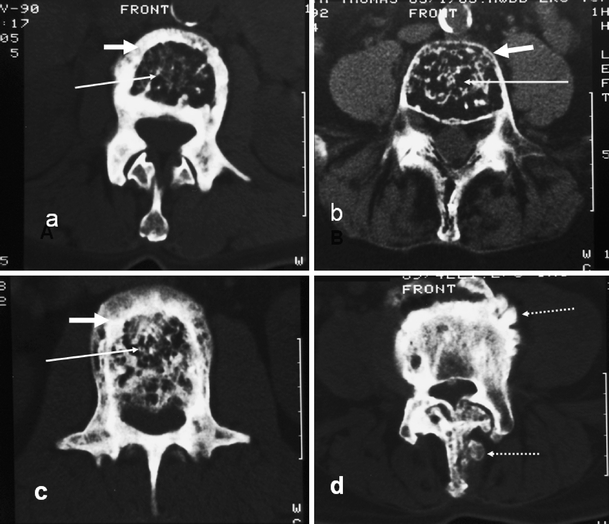
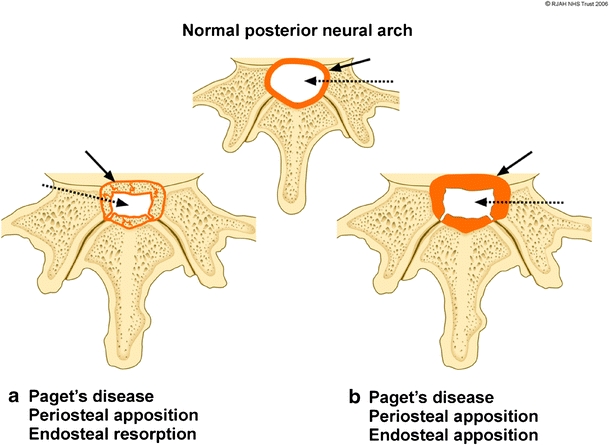
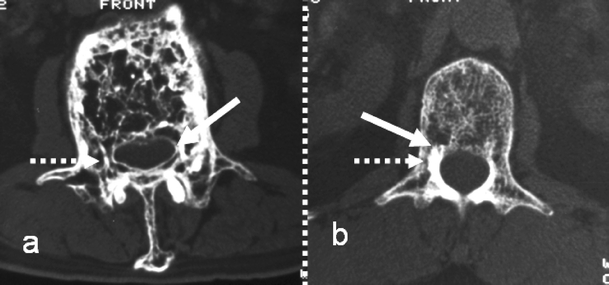
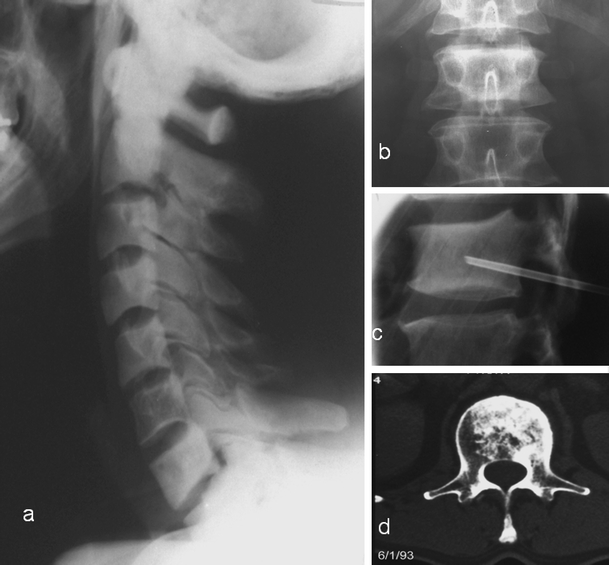
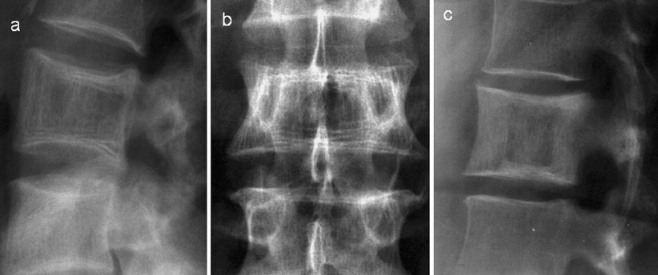
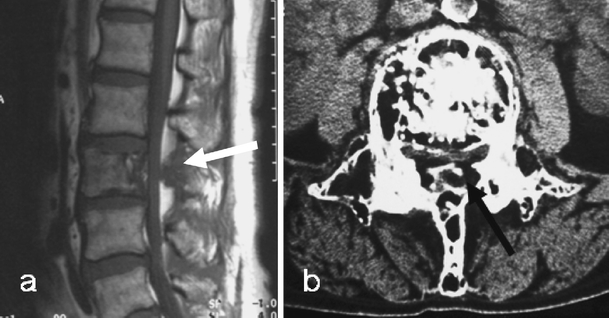
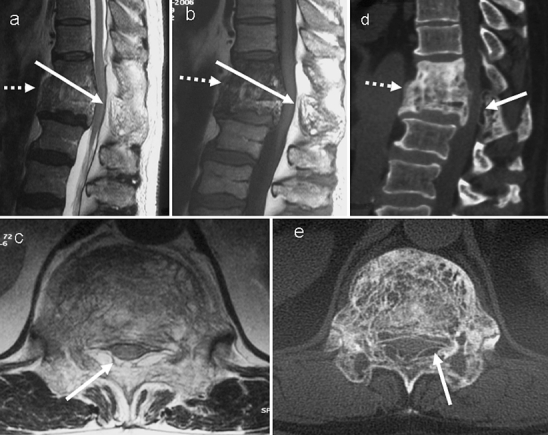
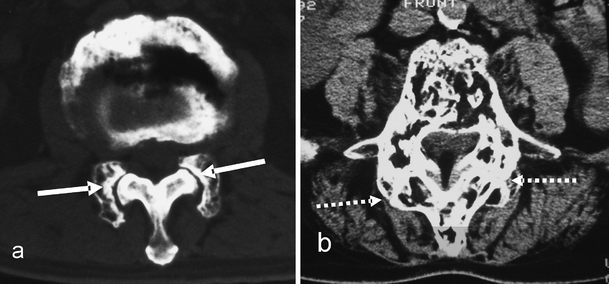
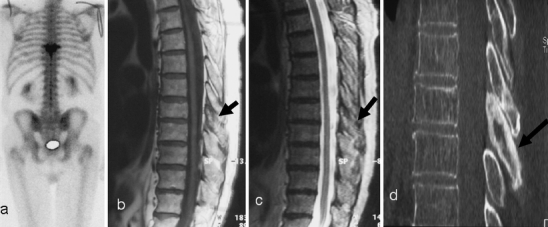
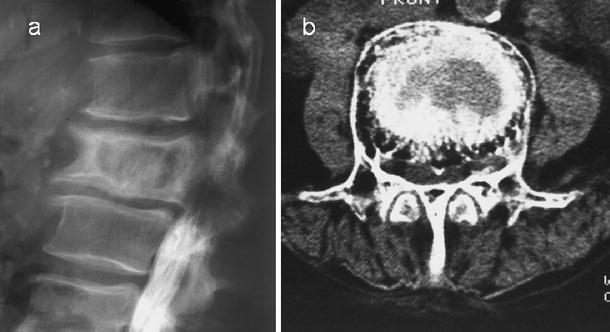
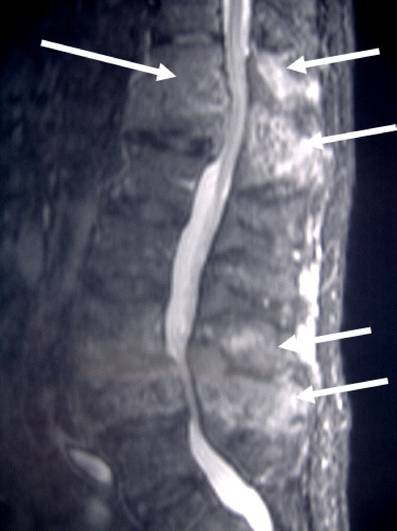
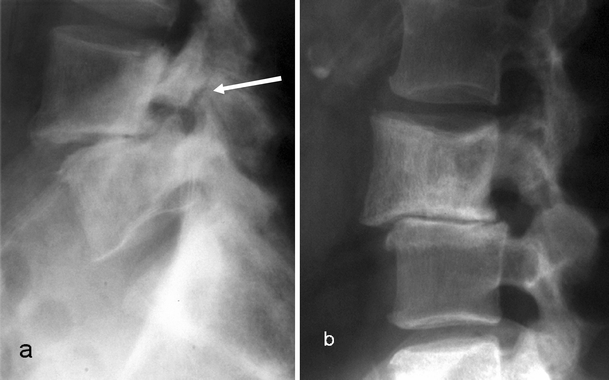
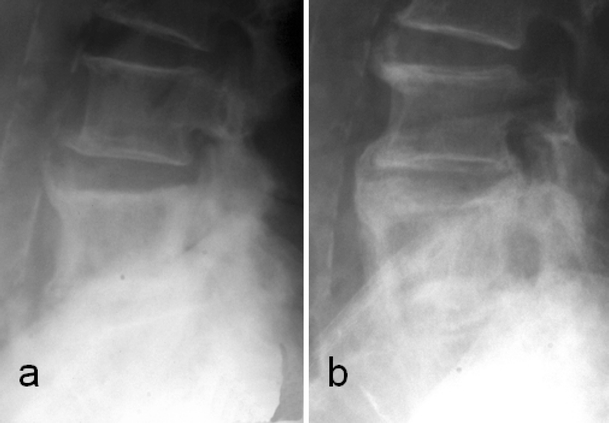
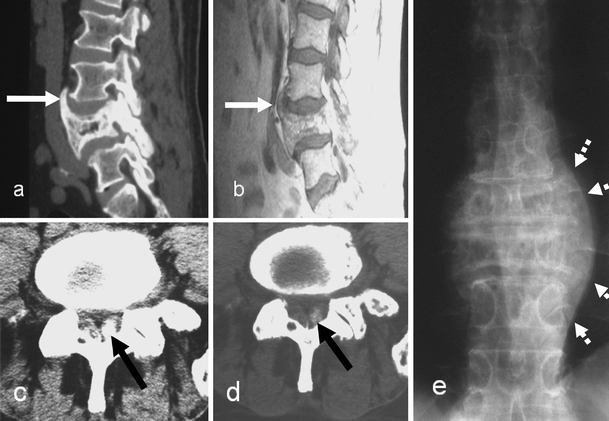
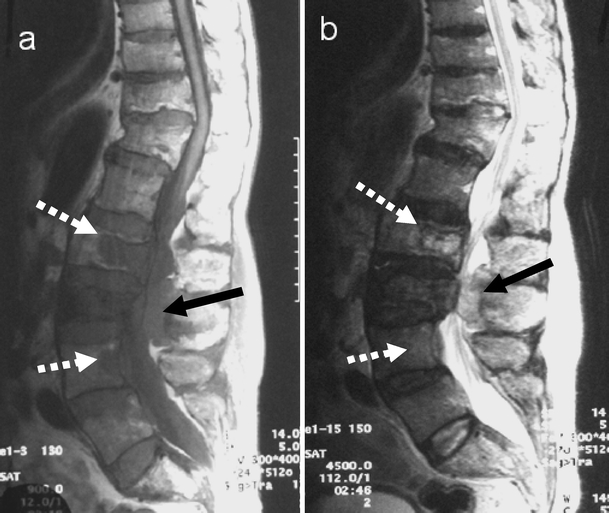
Paget's disease (PD) is a chronic metabolically active bone disease, characterized by a disturbance in bone modelling and remodelling due to an increase in osteoblastic and osteoclastic activity. The vertebra is the second most commonly affected site. This article reviews the various spinal pathomechanisms and osseous dynamics involved in producing the varied imaging appearances and their clinical relevance. Advanced imaging of osseous, articular and bone marrow manifestations of PD in all the vertebral components are presented. Pagetic changes often result in clinical symptoms including back pain, spinal stenosis and neural dysfunction. Various pathological complications due to PD involvement result in these clinical symptoms. Recognition of the imaging manifestations of spinal PD and the potential complications that cause the clinical symptoms enables accurate assessment of patients prior to appropriate management.
Figures




References
-
- Schmorl G. Über Osteitis deformans Paget. Virchows Arch Pathol Anat Physiol 1932; 238: 694–751. - DOI
-
- Maldague B, Malghem J. Dynamic radiologic patterns of Paget’s disease of bone. Clin Orthop Relat Res 1987; 217: 126–151. - PubMed
-
- Basle MF, Rebel A, Fournier JG, Russell WC, Malkani K. On the trail of paramyxoviruses in Paget’s disease of bone. Clin Orthop Relat Res 1987; 217: 9–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
