

The ratio between metastatic and examined lymph nodes (N ratio) is an independent prognostic factor in gastric cancer regardless of the type of lymphadenectomy: results from an Italian multicentric study in 1853 patients
- PMID: 17414602
- PMCID: PMC1877031
- DOI: 10.1097/01.sla.0000250423.43436.e1
The ratio between metastatic and examined lymph nodes (N ratio) is an independent prognostic factor in gastric cancer regardless of the type of lymphadenectomy: results from an Italian multicentric study in 1853 patients
Abstract
Purpose: To investigate whether the ratio between metastatic and examined lymph nodes (N ratio) is a better prognostic factor as compared with traditional staging systems in patients with gastric cancer regardless of the extension of lymph node dissection.
Patients & methods: We retrospectively reviewed the data of 1853 patients who underwent radical resection for gastric carcinoma at 6 Italian centers. Patients with >15 (group 1, n = 1421) and those with <or=15 (group 2, n = 432) lymph nodes examined were separately analyzed. N ratio categories (N ratio 0, 0%; N ratio 1, 1%-9%; N ratio 2, 10%-25%; N ratio 3, >25%) were determined by the best cut-off approach.
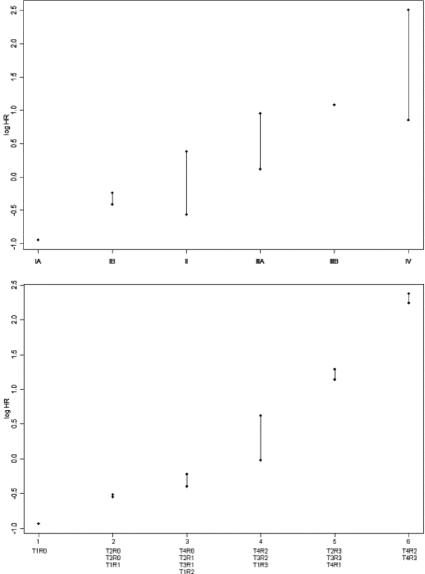
Results: After a median follow-up of 45.5 months (range, 4-182 months), the 5-year overall survival of N0, N1, and N2 patients of group 1 versus group 2 was 83.4% versus 74.2% (P = 0.0026), 54.3% versus 44.3% (P = 0.018), and 32.7% versus 14.7% (P = 0.004), respectively, suggesting that a low number of excised lymph nodes can lead to the understaging of patients. N ratio identified subsets of patients with significantly different survival rates within N1 and N2 stages in both groups. At multivariate analysis, the N ratio (but not N stage) was retained as an independent prognostic factor both in group 1 and group 2 (HR for N ratio 1, N ratio 2, and N ratio 3 = 1.67, 2.96, and 6.59, and 1.56, 2.68, and 4.28, respectively). In our series, the implementation of N ratio led to the identification of subgroups of patients prognostically more homogeneous than those classified by the TNM system.
Conclusion: N ratio is a simple and reproducible prognostic tool that can stratify patients with gastric cancer also in case of limited lymph node dissection. These data may represent the rational for improving the prognostic power of current UICC TNM staging system and ultimately the selection of patients who may most benefit from adjuvant treatments.
Figures

References
-
- Bozzetti F, Bonfanti G, Morabito T, et al. A multifactorial approach for the prognosis of patients with carcinoma of the stomach after curative resection. Surg Gynecol Obstet. 1986;162:229–234. - PubMed
-
- Hohenberger P, Gretschel S. Gastric cancer. Lancet. 2003;362:305–315. - PubMed
-
- Japanese Research Society for Gastric Cancer. The general rules for the gastric cancer study in surgery and pathology. I. Jpn J Surg. 1981;11:127–139. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
