

Case Reports
Reversibility of venous sinus obstruction in idiopathic intracranial hypertension
Affiliations
- PMID: 17416816
- PMCID: PMC7977370
Item in Clipboard
Case Reports
Reversibility of venous sinus obstruction in idiopathic intracranial hypertension
AJNR Am J Neuroradiol.
2007 Apr.
Abstract
Elevated intracranial intravenous pressure seems to be of importance in pseudotumor cerebri syndromes, either as a cause (secondary intracranial hypertension) or as a consequence (idiopathic intracranial hypertension) of increased intracranial pressure. We present 3 case reports in which diagnostic imaging before and after CSF diversion provided evidence that narrowing of the transverse sinuses is a secondary phenomenon. Stent angioplasty of the venous sinuses should not be considered a therapeutic approach in these cases.
Figures
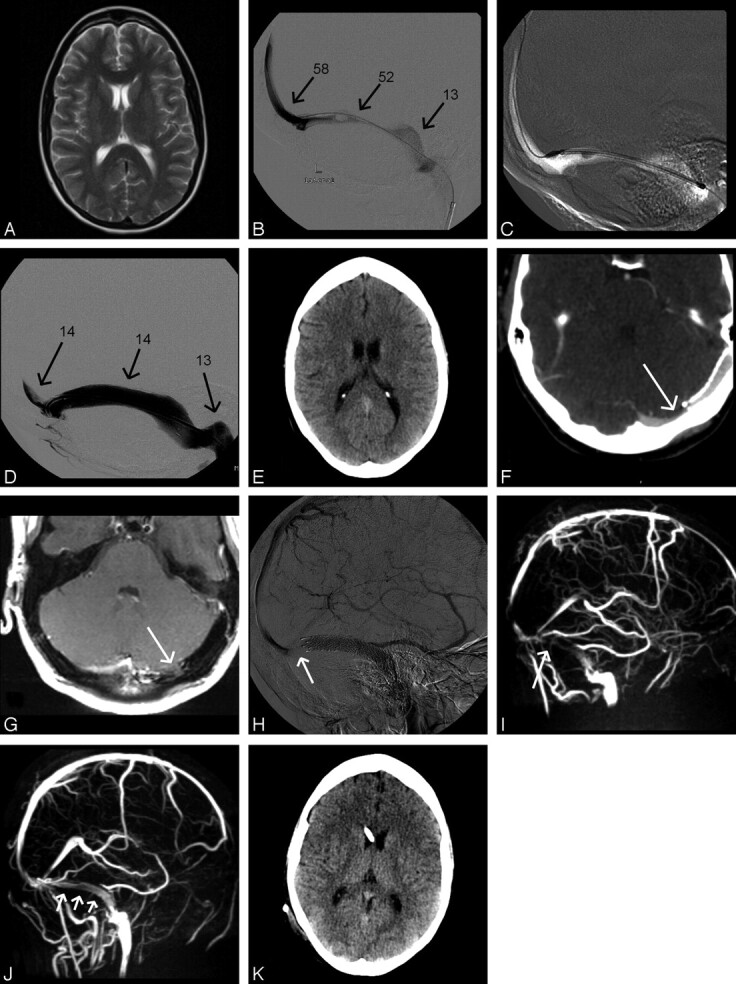
Case 1: A and B, Axial T2-weighted turbo spin-echo (A) and venography (B) using a microcatheter in the torcular herophili inserted through the left TS (arrows, known aplasia of the right TS). The left TS in the lateral projection shows high-grade narrowing distal to a filling defect assumed to be an arachnoid granulation. C, Pressure monitoring at different locations (in centimeters H2O). D, Placement of a self-expanding nitinol stent (Absolute, Guidant, Indianapolis, Ind; 8 mm in diameter, 6-cm in length). Stenosis is abolished after stent placement. E, Poststent placement on routine cranial CT. F and G, On follow-up, contrast-enhanced CT (F) and proton-weighted MR imaging (G) in the same axial section position demonstrate a new stenosis in the medial aspect of the left transverse sinus (arrows) proximal to the stent. H and I, Venous phase of right internal carotid artery angiography in the lateral projection (H) and maximum intensity projection of MRV in the lateral projection (I) confirm the finding. Arrows indicate pre-stent stenosis. J, Following lumbar puncture, MRV shows significantly better flow signal intensity in the left transverse sinus proximal and within the stent (arrows) with albeit some signal-intensity reduction believed to be due to the stent material. K, Cranial CT after insertion of a ventriculoperitoneal shunt.
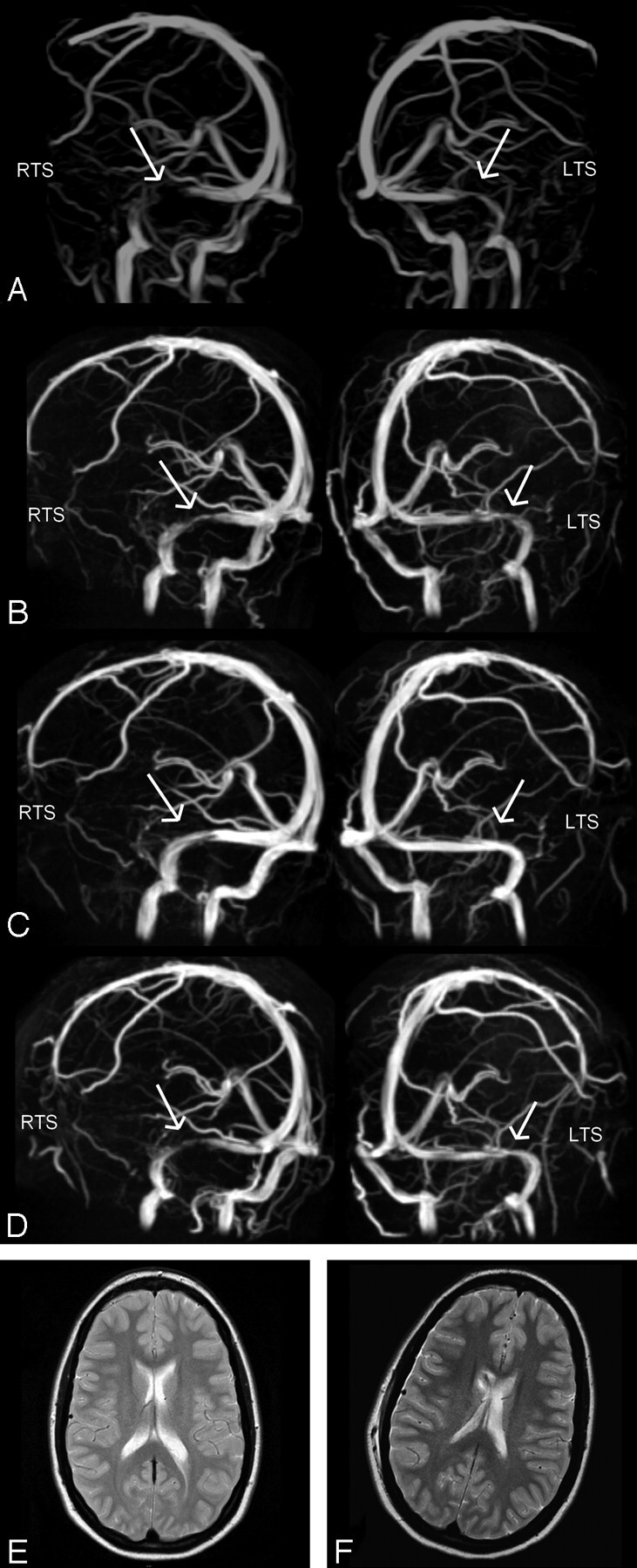
Case 2: MIP of MRV in oblique anteroposterior left and right views obtained at a lumbar CSF pressures of 50 cm H2O (A), after lumbar puncture (B), after a 2nd lumbar puncture with no residual pressure being monitored (C), and after placement of a ventriculoperitoneal shunt (D). Stenoses in both the left and right transverse sinuses (LTS, RTS), as marked with arrows, are reduced in accordance with a lowered CSF pressure, with complete resolution in C. Probably as a result of a relatively high opening pressure of the valve of the ventriculoperitoneal shunt, transverse sinuses show some residual narrowing (D). T2-weighted axial images before (E) and after (F) insertion of a ventriculoperitoneal shunt into the right ventricle show no difference in ventricle size.
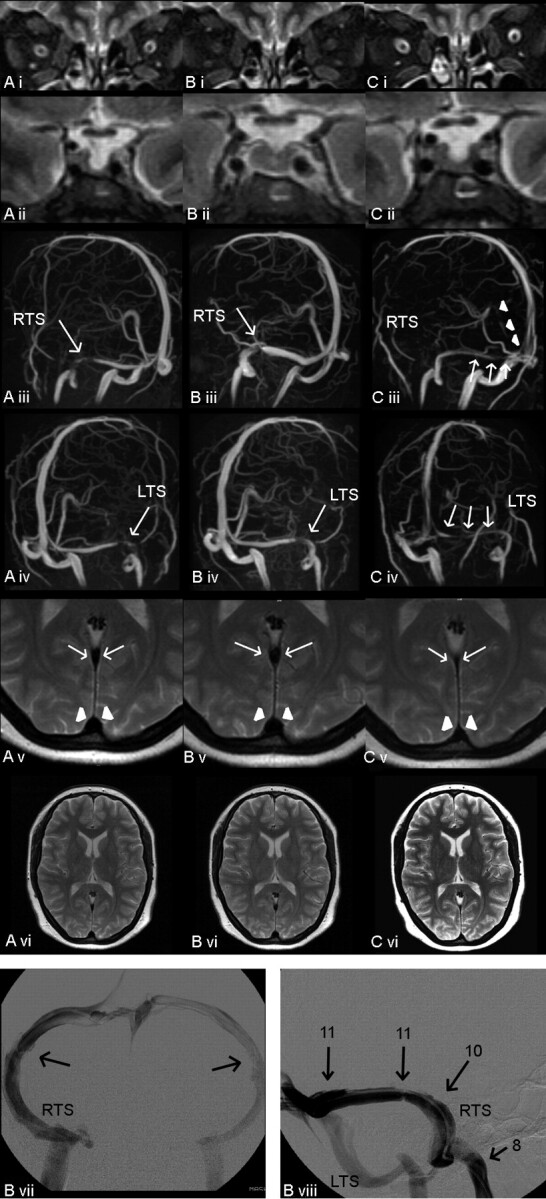
A–C, Case 3: MR imaging, MRV, and conventional venography at different points of time. CSF pressure 30 cm H2O (A); after CSF diversion, pressure of 11 cm H2O (B); and 7 days later (C). Fat-saturated T2-weighted turbo spin-echo inversion-recovery images in the coronal plane (TR/TE, 2650/180; Sl, 3 mm) (i), showing widening of the optic sheathes in A and C (arrows) and partially empty sella in A (ii) and C (ii). MIP of MRV in oblique anteroposterior views demonstrating narrowing of the RTS (iii) and the LTS (iv) (arrows) as well as in the straight sinus (arrowheads). T2-weighted turbo spin-echo images in the axial plane at the level of the straight sinus (arrows) and superior sagittal sinus (arrowheads, v), both being compressed in C. T2-weighted axial images showing normal ventricle size (vi). Conventional venography with the catheter placed in the RTS close to the torcular herophili was performed after CSF diversion (pressure of 11 cm H2O). B vii, Anteroposterior view shows bilateral low-grade TS stenoses. B viii, Lateral tilted view shows intravenous pressure monitoring in the RTS at different locations (arrows, pressure in centimeters H2O).
Comment in
-
Stenoses in idiopathic intracranial hypertension: to stent or not to stent?AJNR Am J Neuroradiol. 2008 Feb;29(2):215; author reply 215-6. doi: 10.3174/ajnr.A0804. AJNR Am J Neuroradiol. 2008. PMID: 18272567 Free PMC article. No abstract available.
References
-
- Binder DK, Horton JC, Lawton MT, et al. Idiopathic intracranial hypertension. Neurosurgery 2004;54:538–52 - PubMed
-
- Karahalios DG, Rekate HL, Khayata MH, et al. Elevated intracranial pressure as a universal mechanism in pseudotumor cerebri of varying etiologies. Neurology 1996;46:198–202 - PubMed
-
- Farb RI, Vanek I, Scott JN, et al. Idiopathic intracranial hypertension: the prevalence and morphology of sinovenous stenosis. Neurology 2003;60:1418–24 - PubMed
-
- Owler BK, Parker G, Halmagyi M, et al. Pseudotumor cerebri syndrome: venous sinus obstruction and its treatment with stent placement. J Neurosurg 2003;98:1045–55 - PubMed
-
- King JO, Mitchell PJ, Thomson KR, et al. Manometry combined with cervical puncture in idiopathic intracranial hypertension. Neurology 2002;58:26–30 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources