

CT angiography and perfusion CT in cerebral vasospasm after subarachnoid hemorrhage
- PMID: 17416833
- PMCID: PMC7977351
CT angiography and perfusion CT in cerebral vasospasm after subarachnoid hemorrhage
Abstract
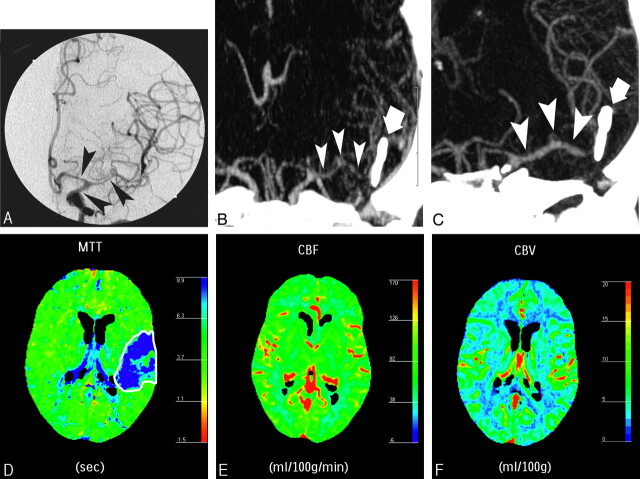
Background and purpose: We investigated the association of multisection CT angiography (MSCTA) and perfusion CT (PCT) for the characterization of vasospasm secondary to aneurysmal subarachnoid hemorrhage.
Materials and methods: Among 27 patients with symptomatic cerebrovascular vasospasm investigated by digital subtraction angiography (DSA), 18 underwent both cerebral PCT and MSCTA. For the remaining 9, only PCT or MSCTA could be performed. MSCTA was compared with DSA for the detection and characterization of vasospasm on 286 intracranial arterial segments. PCT maps were visually reviewed for mean transit time, relative cerebral blood flow, and relative cerebral blood volume abnormalities and were qualitatively compared with the corresponding regional vasospasm detected by DSA.
Results: Vasospasm was grouped into 2 categories: mild-moderate and severe. The depiction of vasospasm by MSCTA showed the best sensitivity, specificity, and accuracy at the level of the A2 and M2 arterial segments (100% for each), in contrast to the carotid siphon (45%, 100%, and 85% respectively). The characterization of vasospasm severity by MSCTA showed a sensitivity, specificity, and accuracy of 86.8%, 96.8%, and 95.2%, respectively, for mild-moderate vasospasm, and 76.5%, 99.5%, and 97.5%, respectively, for severe vasospasm. The PCT abnormalities were related to severe vasospasm in 9 patients and to mild-to-moderate vasospasm in 2. The sensitivity, specificity, and accuracy of PCT in detecting vasospasm were 90%, 100%, and 92.3%, respectively, for severe vasospasm, and 20%, 100%, and 38.5%, respectively, for mild-moderate vasospasm.
Conclusion: MSCTA/PCT can assess the location and severity of cerebrovascular vasospasm and its related perfusion abnormalities. It can identify severe vasospasm with risk of delayed ischemia and can thus guide the invasive treatment.
Figures


References
-
- Kassell NF, Sasaki T, Colohan AR, et al. Cerebral vasospasm following aneurysmal subarachnoid hemorrhage. Stroke 1985;16:562–72 - PubMed
-
- Treggiari-Venzi MM, Suter PM, Romand JA. Review of medical prevention of vasospasm after aneurysmal subarachnoid hemorrhage: a problem of neurointensive care. Neurosurgery 2001;48:249–61 - PubMed
-
- Proust F, Hannequin D, Langlois O, et al. Causes of morbidity and mortality after ruptured aneurysm surgery in a series of 230 patients. The importance of control angiography. Stroke 1995;26:1553–57 - PubMed
-
- Kassel NF, Peerless SJ, Durward QT, et al. Treatment of ischemic deficits from vasospasm with intravascular volume expansion and induced arterial hypertension. Neurosurgery 1982;11:337–47 - PubMed
-
- Shimoda M, Oda S, Tsugane R, et al. Intracranial complications of hypervolemic therapy in patients with a delayed ischemic deficit attributed to vasospasm. J Neurosurg 1993;78:423–29 - PubMed