

Comparison of the modified Early Treatment Diabetic Retinopathy Study and mild macular grid laser photocoagulation strategies for diabetic macular edema
- PMID: 17420366
- PMCID: PMC2536574
- DOI: 10.1001/archopht.125.4.469
Comparison of the modified Early Treatment Diabetic Retinopathy Study and mild macular grid laser photocoagulation strategies for diabetic macular edema
Abstract
Objective: To compare 2 laser photocoagulation techniques for treatment of diabetic macular edema: the modified Early Treatment Diabetic Retinopathy Study (ETDRS) direct/grid photocoagulation technique and a potentially milder (but potentially more extensive) mild macular grid (MMG) laser technique in which microaneurysms are not treated directly and small mild burns are placed throughout the macula, whether or not edema is present.
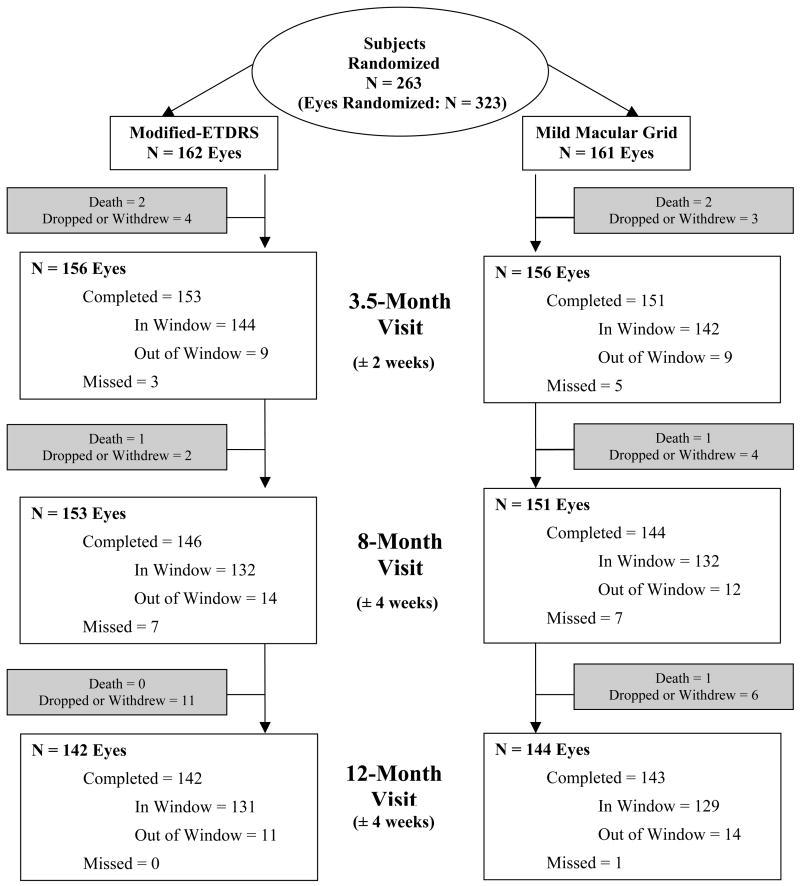
Methods: Two hundred sixty-three subjects (mean age, 59 years) with previously untreated diabetic macular edema were randomly assigned to receive laser photocoagulation by either the modified ETDRS (162 eyes) or MMG (161 eyes) technique. Visual acuity, fundus photographs, and optical coherence tomography measurements were obtained at baseline and at 3.5, 8, and 12 months. Treatment was repeated if diabetic macular edema persisted.
Main outcome measure: Change in optical coherence tomography measurements at 12-month follow-up.
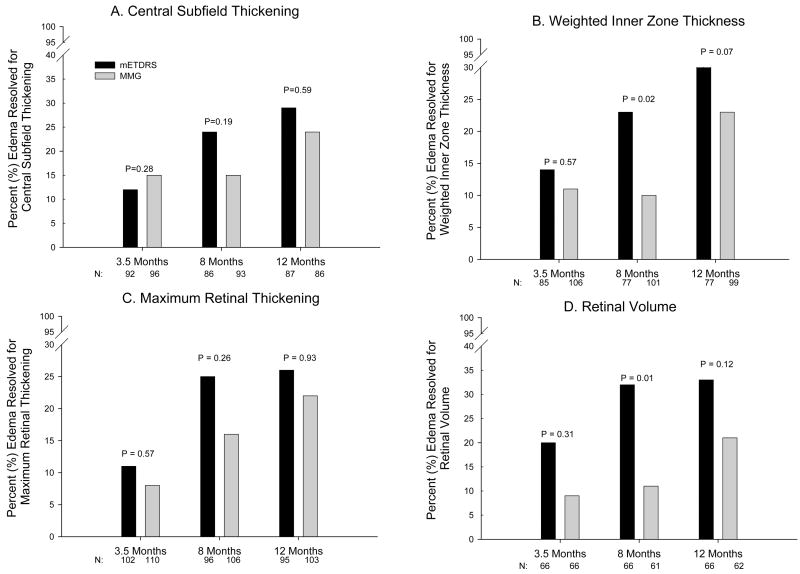
Results: Among eyes with a baseline central subfield thickness of 250 microm or greater, central subfield thickening decreased by an average of 88 microm in the modified ETDRS group and by 49 microm in the MMG group at 12-month follow-up (adjusted mean difference, 33 microm; 95% confidence interval, 5-61 microm; P = .02). Weighted inner zone thickening by optical coherence tomography decreased by 42 microm in the modified ETDRS group and by 28 microm in the MMG group (adjusted mean difference, 14 microm; 95% confidence interval, 1-27 microm; P = .04); maximum retinal thickening (maximum thickening of the central and 4 inner subfields) decreased by 66 and 39 microm, respectively (adjusted mean difference, 27 microm; 95% confidence interval, 6-47 microm; P = .01), and retinal volume decreased by 0.8 and 0.4 mm3, respectively (adjusted mean difference, 0.3 mm3; 95% confidence interval, 0.02-0.53 mm3; P = .03). At 12 months, the mean change in visual acuity was 0 letters in the modified ETDRS group and 2 letters worse in the MMG group (adjusted mean difference, 2 letters; 95% confidence interval, -0.5 to 5 letters; P = .10).
Conclusions: At 12 months after treatment, the MMG technique was less effective at reducing optical coherence tomography-measured retinal thickening than the more extensively evaluated current modified ETDRS laser photocoagulation approach. However, the visual acuity outcome with both approaches is not substantially different. Given these findings, a larger long-term trial of the MMG technique is not justified.
Application to clinical practice: Modified ETDRS focal photocoagulation should continue to be a standard approach for treating diabetic macular edema.
Trial registration: clinicaltrials.gov Identifier: NCT00071773.
Figures
References
-
- Tso MOM, Wallow IHL, Elgin S. Experimental photocoagulation of the human retina. I. Correlation of physical, clinical, and pathologic data. Arch Ophthalmol. 1977;95:1035–40. - PubMed
-
- Apple DJ, Goldberg MF, Wyhinny G. Histopathology and ultrastructure of the argon laser lesion in human retinal and choroidal vasculatures. Am J Ophthalmol. 1973;75:595–609. - PubMed
-
- Wilson DJ, Finkelstein D, Quigley HA, Green WR. Macular grid photocoagulation. An experimental study on the primate retina. Arch Ophthalmol. 1988;106:100–5. - PubMed
-
- Arnarsson A, Stefansson E. Laser treatment and the mechanism of edema reduction in branch retinal vein occlusion. Invest Ophthalmol Vis Sci. 2000;41:877–9. - PubMed
-
- Ogata N, Tombran-Tink J, Jo N, Mrazek D, Matsumura M. Upregulation of pigment epithelium-derived factor after laser photocoagulation. Am J Ophthalmol. 2001;132:427–9. - PubMed
