

Thoracic outlet syndrome: a 50-year experience at Baylor University Medical Center
- PMID: 17431445
- PMCID: PMC1849872
- DOI: 10.1080/08998280.2007.11928267
Thoracic outlet syndrome: a 50-year experience at Baylor University Medical Center
Abstract
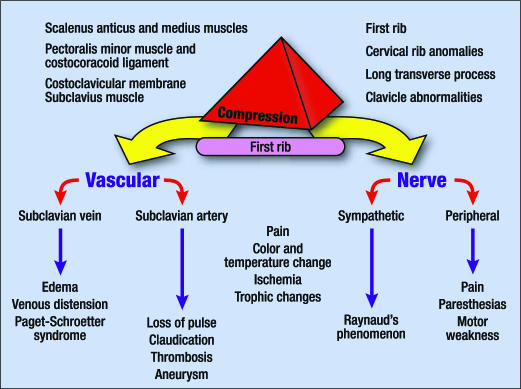
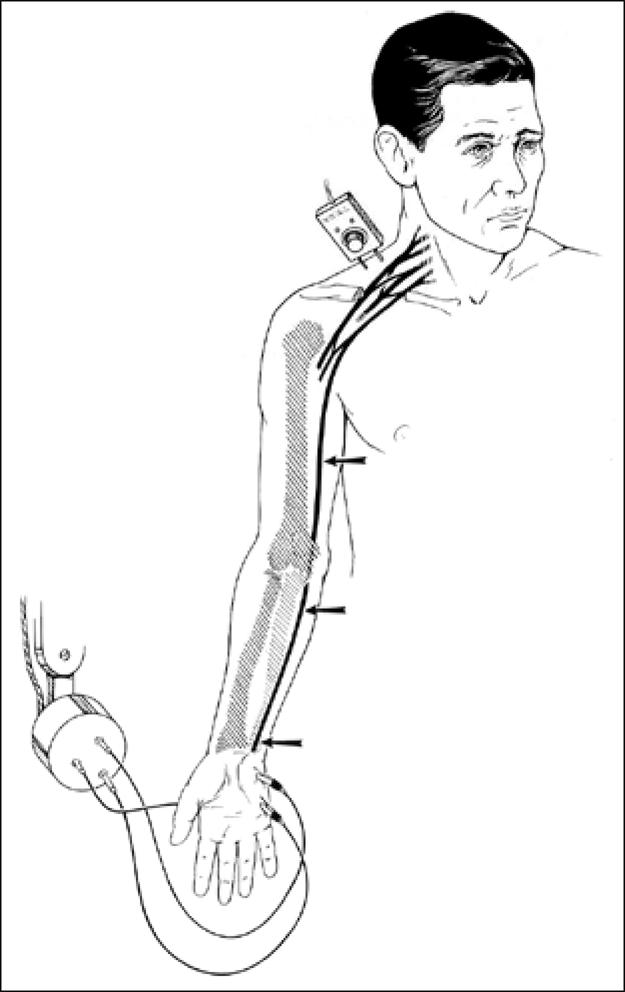
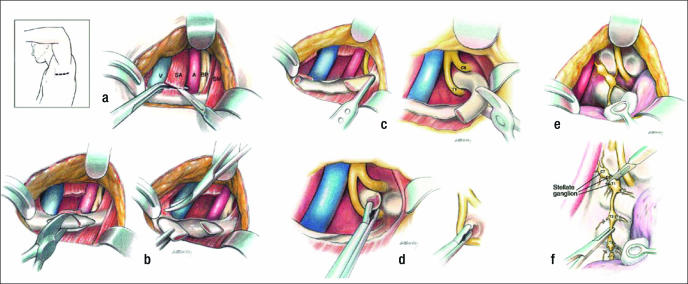
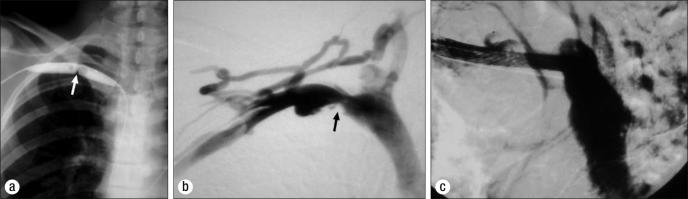
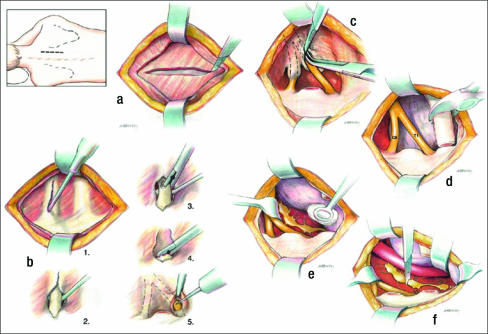
During the past 5 decades, the recognition and management of thoracic outlet syndrome (TOS) have evolved. This article elucidates these changes and improvements in the diagnosis and management of TOS at Baylor University Medical Center. The most remarkable change over the past 50 years is the use of nerve conduction velocity to diagnose and monitor patients with nerve compression. Recognition that procedures such as breast implantation and median sternotomy may produce TOS has been revealing. Prompt thrombolysis followed by surgical venous decompression for Paget-Schroetter syndrome has markedly improved results compared with the conservative anticoagulation approach; thrombolysis and prompt first rib resection is the optimal treatment for most patients with Paget-Schroetter syndrome. Complete first rib extirpation at the initial procedure markedly reduces the incidence of recurrent neurologic symptoms or the need for a second procedure. Chest pain or pseudoangina can be caused by TOS. Dorsal sympathectomy is helpful for patients with sympathetic maintained pain syndrome or causalgia and patients with recurrent TOS symptoms who need a second procedure.
Figures

References
-
- Peet RM, Hendriksen JD, Anderson TP, Martin GM. Thoracic outlet syndrome: evaluation of the therapeutic exercise program. Proc Mayo Clin. 1956;31:281–287. - PubMed
-
- Borchardt M. Symptomatologie und Therapie der Halsrippen. Berl Klin Wochenschr. 1901;38:1265.
-
- Keen WW. The symptomatology, diagnosis and surgical treatment of cervical ribs. Am J Med Sci. 1907;133:173–218.
-
- Coote H. Pressure on the axillary vessels and nerves by an exostosis from a cervical rib; interference with the circulation of the arm; removal of the rib and exostosis, recovery. Med Times Gaz. 1861;2:108.
LinkOut - more resources
Full Text Sources
Miscellaneous