

Review
doi: 10.1053/j.seminhematol.2007.02.004.
Epidemiology and risk factors for venous thrombosis
Affiliations
- PMID: 17433897
- PMCID: PMC2020806
- DOI: 10.1053/j.seminhematol.2007.02.004
Item in Clipboard
Review
Epidemiology and risk factors for venous thrombosis
Semin Hematol.
2007 Apr.
Abstract
Venous thrombosis, including deep vein thrombosis (DVT) and pulmonary embolism (PE), occurs at an annual incidence of about 1 per 1,000 adults. Rates increase sharply after about age 45 years, and are slightly higher in men than women in older age. Major risk factors for thrombosis, other than age, include exogenous factors such as surgery, hospitalization, immobility, trauma, pregnancy, and the puerperium and hormone use, and endogenous factors such as cancer, obesity, and inherited and acquired disorders of hypercoagulation. This review focuses on epidemiology of venous thrombosis and the general implications of this in patient management.
Figures
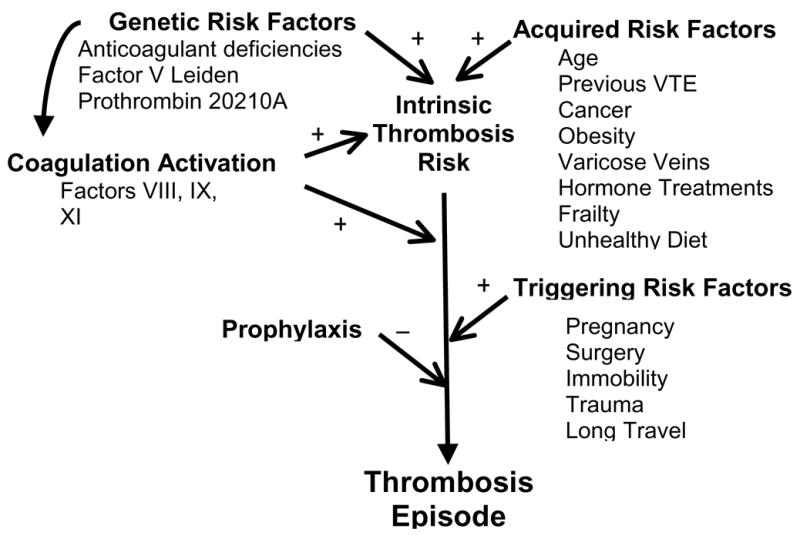
Conceptual framework for the interaction of risk factors in development of venous thrombosis. Intrinsic thrombosis risk is defined by the combinations of genetic and acquired risk factors, including modulation of coagulation activation by known and unknown determinants. The intrinsic risk is altered by the occurrence of triggering risk factors, which can be balanced in appropriate settings by use of thromboprophylaxis.
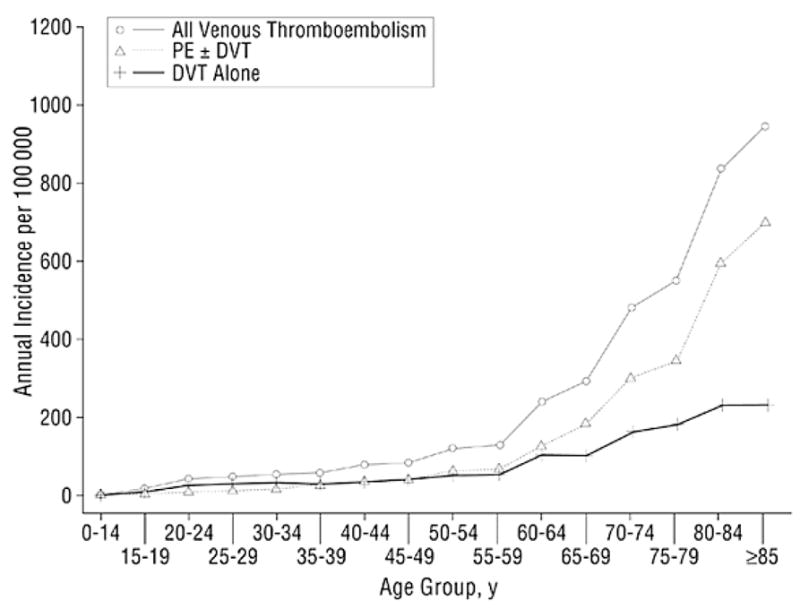
Annual incidence of all venous thromboembolism, deep vein thrombosis (DVT) alone, and pulmonary embolism (PE) with or without deep vein thrombosis (PE ± DVT) among residents of Olmsted County, Minnesota, from 1966 to 1990, by age. Reproduced with permission (6).
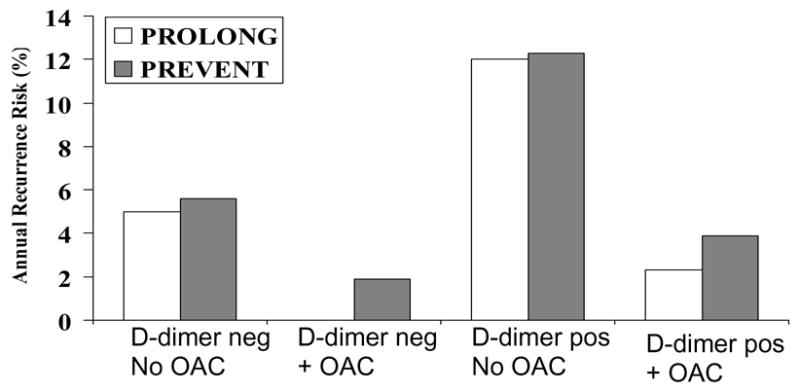
Results from two clinical trials of D-dimer and the risk of recurrent venous thrombosis among patients with idiopathic first events. The PREVENT study randomized patients to low intensity warfarin therapy (target INR 1.5–2.0) and baseline D-dimer elevation was predictive of the risk of recurrent venous thrombosis, regardless of randomized treatment assignment. The lowest rates of recurrence were in the group with low D-dimer on active treatment (67). The PROLONG study was a management study which observed patients with low D-dimer after completing a course of anticoagulation for first thrombosis, and randomized patients with elevated D-dimer to continued anticoagulation or observation. Similar to PREVENT, those with low D-dimer had a lower recurrence risk, and continued anticoagulation was effective in risk reduction among those with elevated D-dimer (70). Pos, positive; neg, negative; OAC, continued long-term oral anticoagulation with vitamin K antagonists.
References
-
- White RH. The epidemiology of venous thromboembolism. Circulation. 2003;107:I-4–I-8. - PubMed
-
- van Korlaar IM, Vossen CY, Rosendaal FR, Bovill EG, Cushman M, Naud S, et al. The impact of venous thrombosis on quality of life. Thromb Res. 2004;114:11–18. - PubMed
-
- Kahn SR, Ducruet T, Lamping DL, Arsenault L, Miron MJ, Roussin A, et al. Prospective evaluation of health-related quality of life in patients with deep venous thrombosis. Arch Intern Med. 2005;165:1173–1178. - PubMed
-
- Cushman M, Tsai AW, White RH, Heckbert SR, Rosamond WD, Enright P, et al. Deep vein thrombosis and pulmonary embolism in two cohorts: the Longitudinal Investigation of Thromboembolism Etiology. Am J Med. 2004;117:19–25. - PubMed
-
- Heit JA, Silverstein MD, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ. Predictors of survival after deep vein thrombosis and pulmonary embolism: a population-based cohort study. Arch Intern Med. 1999;159:445–453. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
