

Monocular activation of V1 and V2 in amblyopic adults measured with functional magnetic resonance imaging
- PMID: 17434776
- PMCID: PMC2174609
- DOI: 10.1016/j.jaapos.2007.01.119
Monocular activation of V1 and V2 in amblyopic adults measured with functional magnetic resonance imaging
Abstract
Purpose: Although previous neuroimaging efforts clearly indicate visual cortical dysfunction in adults with amblyopia, the extent of abnormalities remains unclear.
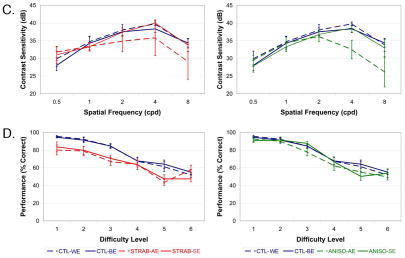
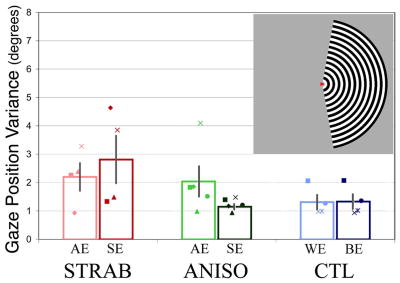
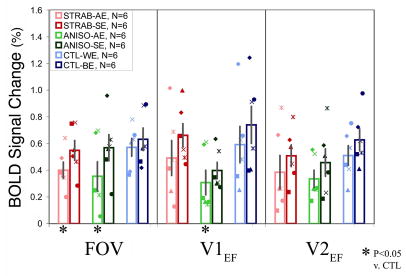
Methods: This functional magnetic resonance imaging (fMRI) study directly compared activity in visual cortex produced by monocular stimulation in 18 adults (six esotropic strabismics, six anisometropes, and six controls). Measures were made in three cortical regions-of-interest, individually defined using standard retinotopic mapping techniques in the nonamblyopic eye, corresponding to extrafoveal V1, extrafoveal V2, and the foveal representation at the occipital pole. Fixation stability was monitored and found not to differ significantly between subject groups.
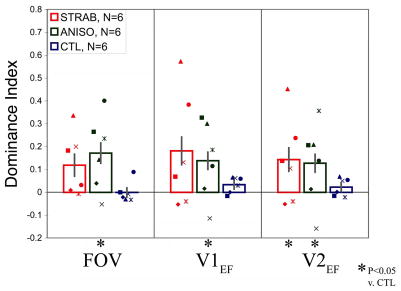
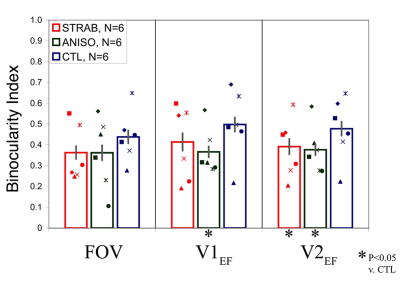
Results: Overall results showed depressed fMRI signal magnitude for amblyopic eyes compared with sound eyes, although a few subjects did not show this trend. Assessment of the spatial extent of activation using an ocular dominance index did show significantly larger interocular differences for both strabismics and anisometropes compared with control subjects for whom eye dominance was carefully defined. In addition, both amblyopic groups showed less cortical area able to be significantly driven by either eye. The magnitude of these effects was equivalent in V1, V2, and the foveal representation, as well as between amblyopic groups. No difference was detected in the strength of signal from the nasal versus temporal retina in either amblyopic group.
Conclusions: Asymmetries in magnitude of monocular activation do occur in subjects with amblyopia, but these basic measures are limited in terms of sensitivity for mild to moderate amblyopia and for specificity between subtypes.
Figures
References
-
- Campos E. Amblyopia. Surv Ophthalmol. 1995 July;40(1):23–39. - PubMed
-
- von Noorden GK, Campos EC. Binocular vision and ocular motility: Theory and management of strabismus. 6. St. Louis: Mosby; 2001.
-
- Daw NW. Critical periods and amblyopia. Arch Ophthalmol. 1998 April;116(4):502–5. - PubMed
-
- Asper L, Crewther D, Crewther SG. Strabismic amblyopia. Part 1. Psychophysics. Clin Exp Optom. 2000 March;83(2):49–58. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
