

Mental training in surgical education: a randomized controlled trial
- PMID: 17435545
- PMCID: PMC1877007
- DOI: 10.1097/01.sla.0000251575.95171.b3
Mental training in surgical education: a randomized controlled trial
Abstract
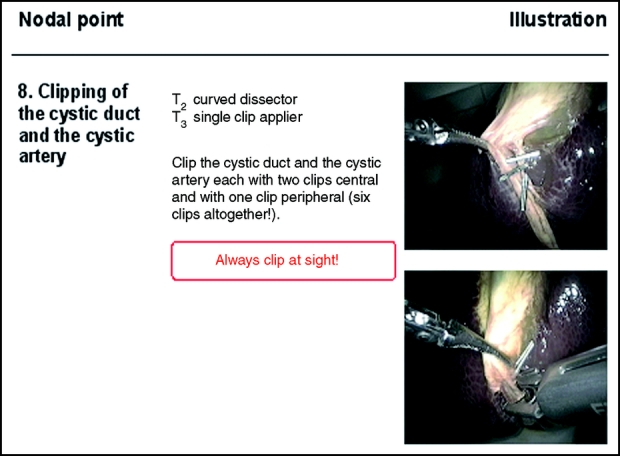
Objective: To evaluate the impact of a cognitive training method on the performance of simulated laparoscopic cholecystectomy in laparoscopic training courses.
Summary background data: Surgeons are like professional sportsmen in that they have to be able to perform complicated, fine-motor movements under stressful conditions. Mental training, systematically and repeatedly imagining a movement's performance, is a well-established technique in sports science, and this study aimed to determine its value in training surgeons.
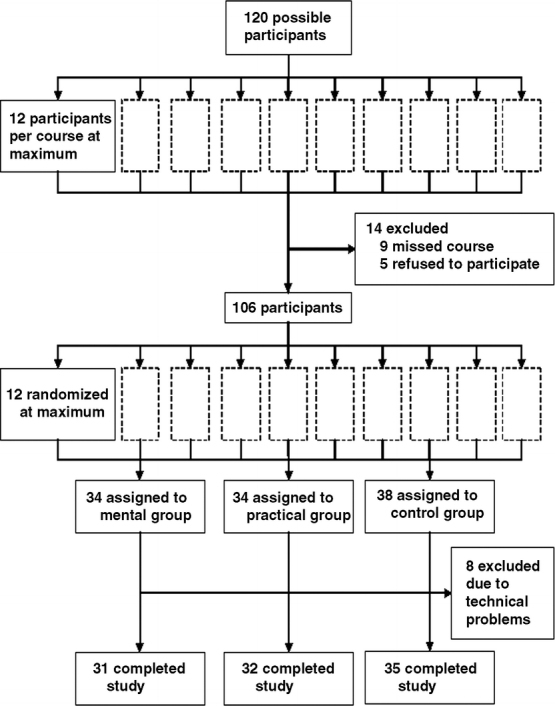
Methods: A total of 98 surgeons undergoing basic laparoscopic training participated in a randomized controlled trial; 31 received additional mental training, 32 additional practical training, and 35 received no additional training (control group). All used a Pelvi-Trainer simulator to perform laparoscopic cholecystectomy at baseline and follow-up, after any additional intervention. We used a modified Objective Structured Assessment of Technical Skills (OSATS) instrument to assess performance. Principle outcome variables were the OSATS task-specific checklist (11 procedural steps, scored as correctly [1] or wrongly [0] performed) and the global rating scale (an overall performance evaluation, scored 1-5).
Results: Improvement in the task-specific checklist score between baseline and follow-up differed significantly between groups (P = 0.046 on ANOVA). Least significant difference tests yielded differences between the mental and practical training groups (P = 0.024) and between the mental training and control groups (P = 0.040), but not between the practical training and control groups (P = 0.789). Paired Student t test showed that performance at follow-up was significantly better in the mental training and control groups (mental training group, P = 0.001; control group, P = 0.018) but not the practical training group (P = 0.342). There were no significant intergroup differences in global rating scale results.
Conclusion: Additional mental training is an effective way of optimizing the outcomes of further training for laparoscopic cholecystectomy. It is associated with fewer costs and with better outcomes in some crucial assessment scales than additional practical training.
Figures
Comment in
-
Mental training in surgical education: a randomized controlled trial.Ann Surg. 2007 Jun;245(6):1002. doi: 10.1097/SLA.0b013e31805d0893. Ann Surg. 2007. PMID: 17522530 Free PMC article. No abstract available.
-
Mental training in surgical education.Ann Surg. 2007 Dec;246(6):1118; author reply 1118-9. doi: 10.1097/SLA.0b013e31815c29b1. Ann Surg. 2007. PMID: 18043123 No abstract available.
References
-
- Holden JG, Flach JM, Donchin Y. Perceptual-motor coordination in an endoscopic surgery simulation. Surg Endosc. 1999;13:127–132. - PubMed
-
- Driskell J, Copper C, Moran A. Does mental practice enhance performance? J Appl Sport Psychol. 1994;79:481–492.
-
- Feltz DL, Landers DM. The effects of mental practice on motor skill learning and performance: a meta-analysis. J Sport Psychol. 1983;5:25–57.
-
- Immenroth M. Mental practice in surgery: some facts. In: Meyer G, Schildberg FW, eds. Complications in Minimal Invasive Surgery: Prevention, Detection, and Treatment. Heidelberg: Springer, In press.
-
- Jänes A. Clipples Laparoscopic Cholecystectomy with Harmonic™. In: Immenroth M, Berg T, Bürger T & Brenner J, eds. Operation Primer (Volume 1). London: Euromed Communications, 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
