

Enteral vancomycin controls methicillin-resistant Staphylococcus aureus endemicity in an intensive care burn unit: a 9-year prospective study
- PMID: 17435547
- PMCID: PMC1877020
- DOI: 10.1097/01.sla.0000250418.14359.31
Enteral vancomycin controls methicillin-resistant Staphylococcus aureus endemicity in an intensive care burn unit: a 9-year prospective study
Abstract
Objective: The aim of this study was to assess the efficacy and safety of enteral vancomycin in controlling MRSA endemicity in an intensive care burn unit.
Summary background data: MRSA is a serious clinical and epidemiologic problem. It is not uncommon that the traditional maneuvers, detection and isolation of carriers, fail to control endemicity due to MRSA.
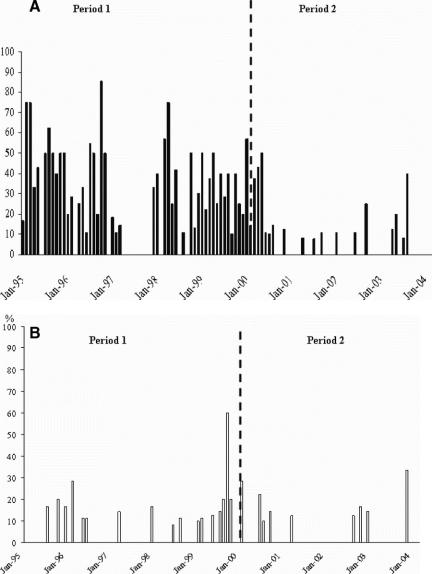
Methods: All patients admitted to an Intensive Care Burn unit from January 1995 to February 2004 have been included in this prospective cohort study comprised 2 different periods. During period 1 (January 1995 to January 2000), barrier and isolation measures were enforced. During period 2 (February 2000 to February 2004), patients received enteral vancomycin 4 times daily in addition to selective digestive decontamination.
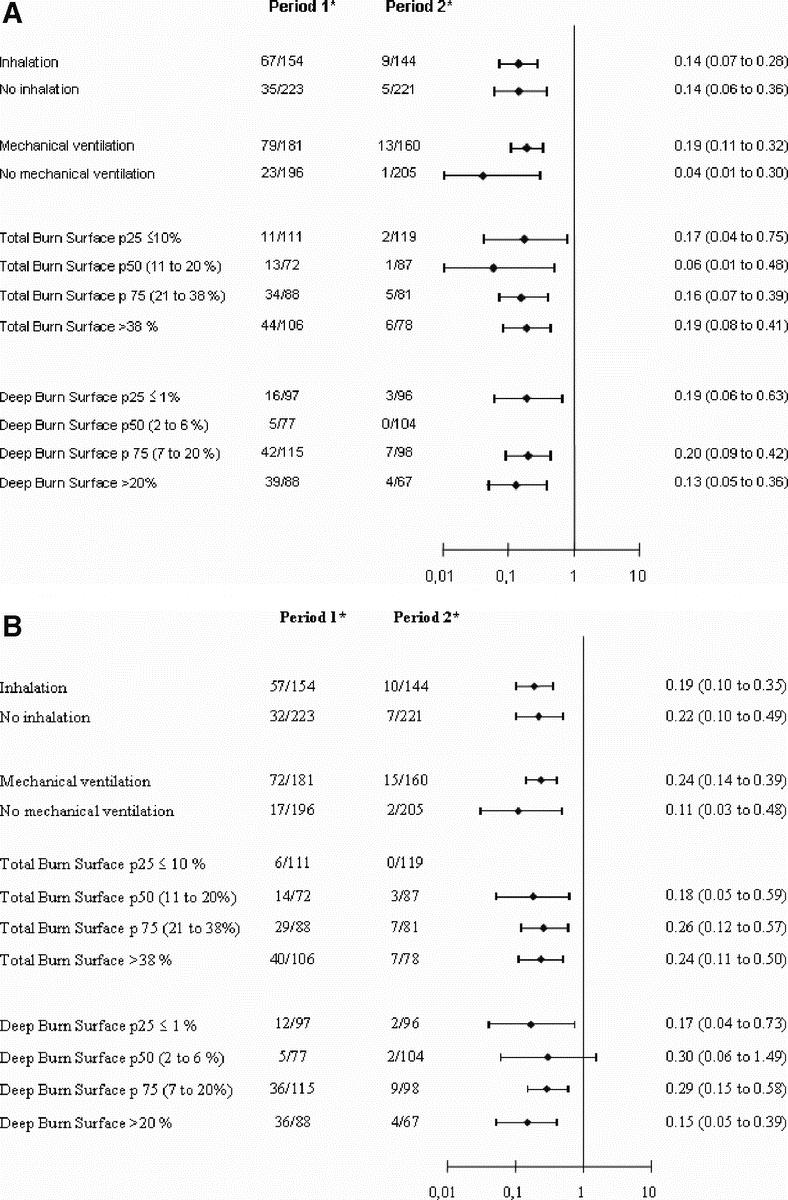
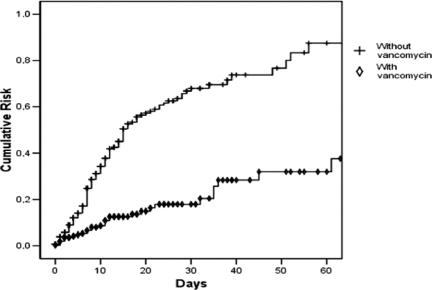
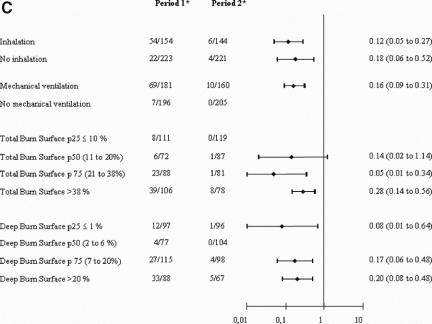
Results: A total of 777 patients were enrolled into the study: 402 in period 1, and 375 in period 2. There were no significant differences in the characteristics of patients between the 2 periods, except for the total body surface burned area, 30.3% in period 1 and 25.61% in period 2 (P = 0.009). There was a significant reduction in the incidence of patients who acquired MRSA from 115 in period 1 to 25 in period 2 (RR, 0.22; 95% confidence interval [CI], 0.15-0.34). Similar reductions were observed in the number of patients with wound (RR, 0.20; 95% CI, 0.12-0.32), blood (RR, 0.13; 95% CI, 0.04-0.35), and tracheal aspirate (RR, 0.07; 95% CI, 0.03-0.19), samples positive for MRSA. There was no emergence of either vancomycin-resistant enterococci or Staphylococcus aureus with intermediate sensitivity to glycopeptides in period 2.
Conclusions: Enteral vancomycin is an effective and safe method to control MRSA in intensive care burn units without VRE.
Figures
Similar articles
-
Effectiveness and safety of enteral vancomycin to control endemicity of methicillin-resistant Staphylococcus aureus in a medical/surgical intensive care unit.J Hosp Infect. 2004 Mar;56(3):175-83. doi: 10.1016/j.jhin.2003.09.021. J Hosp Infect. 2004. PMID: 15003664
-
Topical oropharyngeal vancomycin to control methicillin-resistant Staphylococcus aureus lower airway infection in ventilated patients.Minerva Anestesiol. 2010 Mar;76(3):193-202. Minerva Anestesiol. 2010. PMID: 20203547
-
Use of surveillance cultures and enteral vancomycin to control methicillin-resistant Staphylococcus aureus in a paediatric intensive care unit.Clin Microbiol Infect. 2006 Jan;12(1):35-42. doi: 10.1111/j.1469-0691.2005.01292.x. Clin Microbiol Infect. 2006. PMID: 16460544
-
Selective digestive tract decontamination--will it prevent infection with multidrug-resistant gram-negative pathogens but still be applicable in institutions where methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci are endemic?Clin Infect Dis. 2006 Sep 1;43 Suppl 2:S70-4. doi: 10.1086/504482. Clin Infect Dis. 2006. PMID: 16894518 Review.
-
Vancomycin for surgical prophylaxis?Clin Infect Dis. 2012 May;54(10):1474-9. doi: 10.1093/cid/cis027. Epub 2012 Feb 10. Clin Infect Dis. 2012. PMID: 22328468 Review.
Cited by
-
Intestinal carriage of Staphylococcus aureus: how does its frequency compare with that of nasal carriage and what is its clinical impact?Eur J Clin Microbiol Infect Dis. 2009 Feb;28(2):115-27. doi: 10.1007/s10096-008-0602-7. Epub 2008 Aug 8. Eur J Clin Microbiol Infect Dis. 2009. PMID: 18688664 Review.
-
Selective digestive tract decontamination implementation.Intensive Care Med. 2024 Oct;50(10):1688-1691. doi: 10.1007/s00134-024-07500-w. Epub 2024 Jun 27. Intensive Care Med. 2024. PMID: 38935272 No abstract available.
-
Enteral Vancomycin to Eliminate MRSA Carriership of the Digestive Tract in Critically Ill Patients.Antibiotics (Basel). 2022 Feb 17;11(2):263. doi: 10.3390/antibiotics11020263. Antibiotics (Basel). 2022. PMID: 35203865 Free PMC article.
-
Implementing the MRSA recommendations made by the Commission for Hospital Hygiene and Infection Prevention (KRINKO) of 1999 - current considerations by the DGKH Management Board.GMS Krankenhhyg Interdiszip. 2009 Apr 9;4(1):Doc02. doi: 10.3205/dgkh000127. GMS Krankenhhyg Interdiszip. 2009. PMID: 20204102 Free PMC article.
-
Limiting the spread of highly resistant hospital-acquired microorganisms via critical care transfers: a simulation study.Intensive Care Med. 2011 Oct;37(10):1633-40. doi: 10.1007/s00134-011-2341-y. Epub 2011 Aug 18. Intensive Care Med. 2011. PMID: 21850532 Free PMC article.
References
-
- Deitch EA. The management of burns. N Engl J Med. 1990;323:1249–1253. - PubMed
-
- Pruitt BJ, McManus AT. The changing epidemiology of infection in burn patients. World J Surg. 1992;16:57–67. - PubMed
-
- O'Sullivan ST, O'Connor TPF. Immunosuppression following thermal injury: the pathogenesis of immunodysfunction. Br J Plast Surg. 1997;50:615–623. - PubMed
-
- Rue LW III, Cioffi WG, Mason AD Jr, et al. The risk of pneumonia in thermally injured patients requiring ventilatory support. J Burn Care Rehabil. 1995;16:262–268. - PubMed
-
- de la Cal MA, Cerda E, Garcia-Hierro P, et al. Pneumonia in patients with severe burns: a classification according to the concept of the carrier state. Chest. 2001;119:1160–1165. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
