

A declining rate of completion axillary dissection in sentinel lymph node-positive breast cancer patients is associated with the use of a multivariate nomogram
- PMID: 17435554
- PMCID: PMC1877014
- DOI: 10.1097/01.sla.0000250439.86020.85
A declining rate of completion axillary dissection in sentinel lymph node-positive breast cancer patients is associated with the use of a multivariate nomogram
Abstract
Objective: To compare sentinel lymph node (SLN)-positive breast cancer patients who had completion axillary dissection (ALND) with those who did not, with particular attention to clinicopathologic features, nomogram scores, rates of axillary local recurrence (LR), and changes in treatment pattern over time.
Background: While conventional treatment of SLN-positive patients is to perform ALND, there may be a low-risk subgroup of SLN-positive patients in whom ALND is not required. A multivariate nomogram that predicts the likelihood of residual axillary disease may assist in identifying this group.
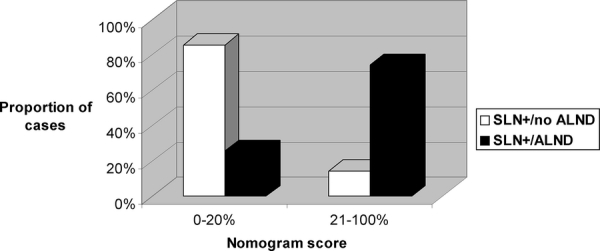
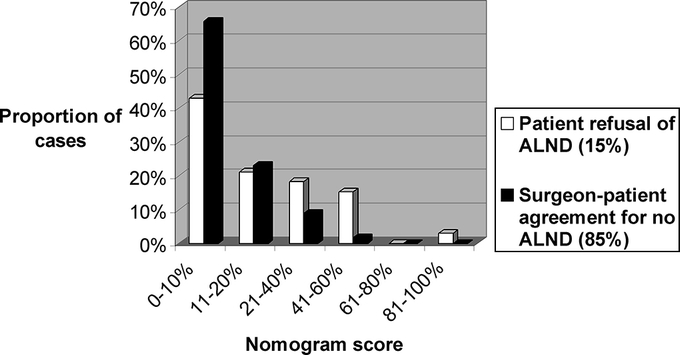
Methods: Among 1960 consecutive SLN-positive patients (1997-2004), 1673 (85%) had ALND ("SLN+/ALND") and 287 (15%) did not ("SLN+/no ALND"). We compare in detail the clinicopathologic features, nomogram scores, and rates of axillary LR between groups.
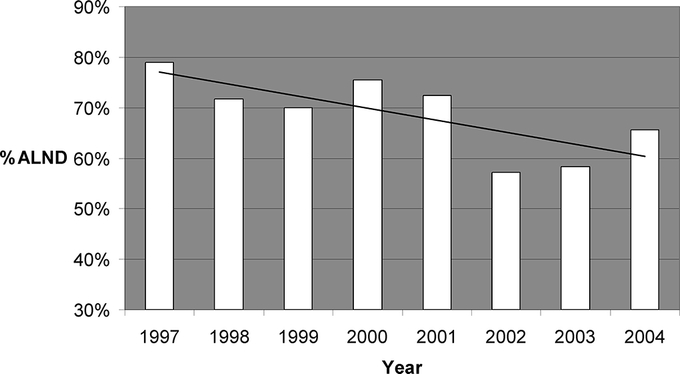
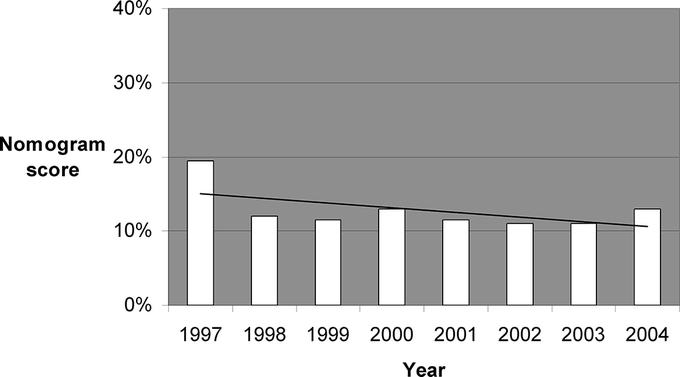
Results: Compared with the SLN+/ALND group, patients with SLN+/no ALND were older, had more favorable tumors, were more likely to have breast conservation, had a lower median predicted risk of residual axillary node metastases (9% vs. 37%, P < 0.001), and had a marginally higher rate of axillary LR (2% vs. 0.4%, P = 0.004) at 23 to 30 months' follow-up; half of all axillary LR in SLN+/no ALND patients were coincident with other local or distant sites. For patients in whom intraoperative frozen section was either negative or not done, the rate of completion ALND declined from 79% in 1997 to 62% in 2003 to 2004 but varied widely by surgeon, ranging from 37% to 100%. For 10 of 10 evaluable surgeons, the median nomogram scores in the SLN+/no ALND group were <or=10.5.
Conclusions: SLN+/no ALND breast cancer patients, a selected group with relatively favorable disease characteristics, had a 9% predicted likelihood of residual axillary disease by nomogram but an observed axillary LR of 2%. A gradual and significant decline over time in the rate of completion ALND is associated with, but not entirely explained by, the institution of a predictive nomogram. It is reasonable to omit ALND for a low-risk subset of SLN-positive patients.
Figures
References
-
- Veronesi U, Paganelli G, Viale G, et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. N Engl J Med. 2003;349:546–553. - PubMed
-
- Wilke LG, McCall LM, Posther KE, et al. Surgical complications associated with sentinel lymph node biopsy: results from a prospective international cooperative group trial. Ann Surg Oncol. 2006;13:491–500. - PubMed
-
- Temple LK, Baron R, Cody HS III, et al. Sensory morbidity after sentinel lymph node biopsy and axillary dissection: a prospective study of 233 women. Ann Surg Oncol. 2002;9:654–662. - PubMed
-
- Kim T, Giuliano AE, Lyman GH. Lymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinoma. Cancer. 2006;106:4–16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
