

The extended learning curve for laparoscopic fundoplication: a cohort analysis of 400 consecutive cases
- PMID: 17436134
- PMCID: PMC1852390
- DOI: 10.1007/s11605-007-0132-0
The extended learning curve for laparoscopic fundoplication: a cohort analysis of 400 consecutive cases
Abstract
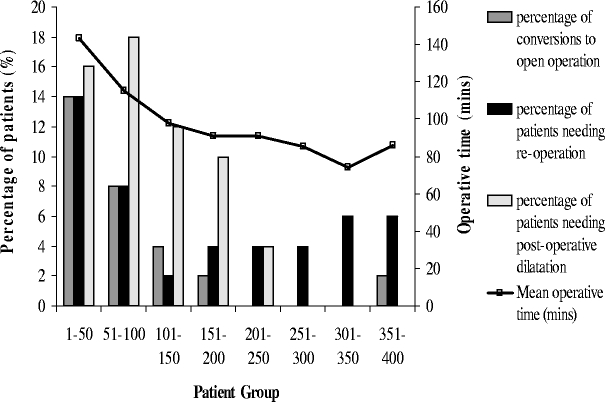
Many studies have looked at the learning curve associated with laparoscopic Nissen fundoplication (LNF) in a given institution. This study looks at the learning curve of a single surgeon with a large cohort of patients over a 10-year period. Prospective data were collected on 400 patients undergoing laparoscopic fundoplication for over 10 years. The patients were grouped consecutively into cohorts of 50 patients. The operating time, the length of postoperative hospital stay, the conversion rate to open operation, the postoperative dilatation rate, and the reoperation rate were analyzed. Results showed that the mean length of operative time decreased from 143 min in the first 50 patients to 86 min in the last 50 patients. The mean postoperative length of hospital stay decreased from 3.7 days initially to 1.2 days latterly. There was a 14% conversion to open operation rate in the first cohort compared with a 2% rate in the last cohort. Fourteen percent of patients required reoperation in the first cohort and 6% in the last cohort. Sixteen percent required postoperative dilatation in the first cohort. None of the last 150 patients required dilatation. In conclusion, laparoscopic fundoplication is a safe and effective operation for patients with gastroesophageal reflux disease. New techniques and better instrumentation were introduced in the early era of LNF. The learning curve, however, continues well beyond the first 20 patients.
Figures
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '10414540', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10414540/'}]}
- Voitk A, Joffe J, Alvarez C, Rosenthal G. Factors contributing to laparoscopic failure during the learning curve for laparoscopic Nissen fundoplication in a community hospital. J Laparoendosc Adv Surg Tech 1999;9:243–248. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00000658-199608000-00013', 'is_inner': False, 'url': 'https://doi.org/10.1097/00000658-199608000-00013'}, {'type': 'PMC', 'value': 'PMC1235342', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC1235342/'}, {'type': 'PubMed', 'value': '8757384', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8757384/'}]}
- Watson DI, Baigrie RJ, Jamieson G. A learning curve for laparoscopic fundoplication. Definable, avoidable, or a waste of time? Ann Surg 1996;224:198–203. - PMC - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1046/j.1365-2168.89.s.1.14_5.x', 'is_inner': False, 'url': 'https://doi.org/10.1046/j.1365-2168.89.s.1.14_5.x'}, {'type': 'PubMed', 'value': '18076018', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/18076018/'}]}
- Booth M, Stratford J, Jones L, Dehn T. Initial results of a randomised trial of laparoscopic total (NISSEN) versus posterior partial (TOUPET) fundoplication for gastro-oesophageal reflux disease (Abstract). Br J Surg 2002;89(Supp1):36. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '1669393', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/1669393/'}]}
- Dallemange B, Weerts JM, Jehaes C, Markiewicz S, Lombard R. Laparoscopic Nissen fundoplication: preliminary report. Surg Laparosc Endosc 1991;1:138–143. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1007/s004640000346', 'is_inner': False, 'url': 'https://doi.org/10.1007/s004640000346'}, {'type': 'PubMed', 'value': '11395813', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11395813/'}]}
- Watson DI, De Beaux AC. Complications of anti-reflux surgery: review article. Surg Endosc 2001;15:344–352. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
