

Risk of fecal diversion in complicated perianal Crohn's disease
- PMID: 17436140
- PMCID: PMC1852374
- DOI: 10.1007/s11605-006-0029-3
Risk of fecal diversion in complicated perianal Crohn's disease
Abstract
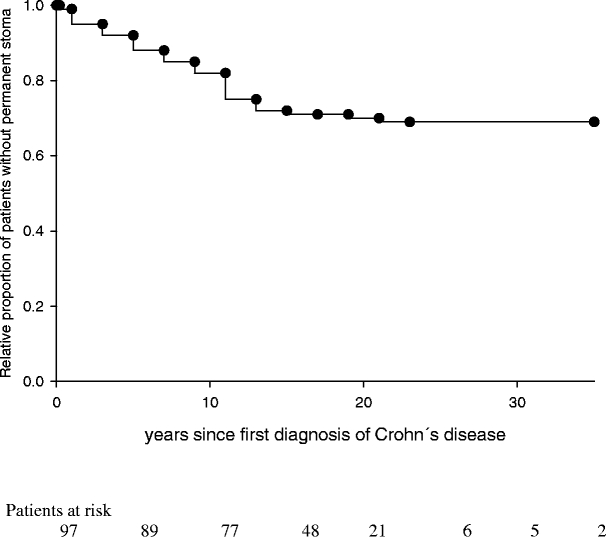
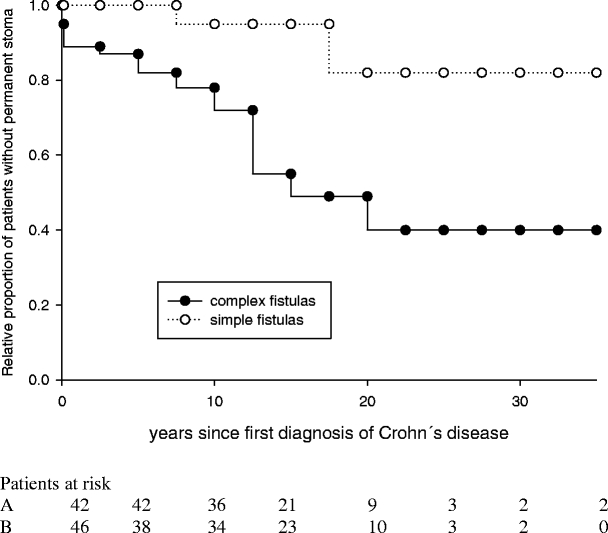
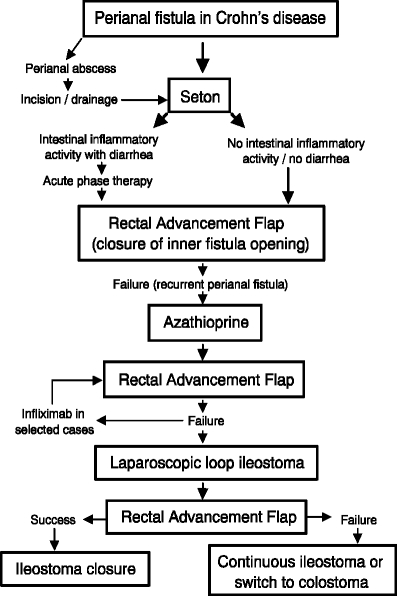
The purpose of the study was to determine the overall risk of a permanent stoma in patients with complicated perianal Crohn's disease, and to identify risk factors predicting stoma carriage. A total of 102 consecutive patients presented with the first manifestation of complicated perianal Crohn's disease in our outpatient department between 1992 and 1995. Ninety-seven patients (95%) could be followed up at a median of 16 years after first diagnosis of Crohn's disease. Patients were sent a standardized questionnaire and patient charts were reviewed with respect to the recurrence of perianal abscesses or fistulas and surgical treatment, including fecal diversion. Factors predictive of permanent stoma carriage were determined by univariate and multivariate analysis. Thirty of 97 patients (31%) with complicated perianal Crohn's disease eventually required a permanent stoma. The median time from first diagnosis of Crohn's disease to permanent fecal diversion was 8.5 years (range 0-23 years). Temporary fecal diversion became necessary in 51 of 97 patients (53%), but could be successfully removed in 24 of 51 patients (47%). Increased rates of permanent fecal diversion were observed in 54% of patients with complex perianal fistulas and in 54% of patients with rectovaginal fistulas, as well as in patients that had undergone subtotal colon resection (60%), left-sided colon resection (83%), or rectal resection (92%). An increased risk for permanent stoma carriage was identified by multivariate analysis for complex perianal fistulas (odds ratio [OR] 5; 95% confidence interval [CI] 2-18), temporary fecal diversion (OR 8; 95% CI 2-35), fecal incontinence (OR 21, 95% CI 3-165), or rectal resection (OR 30; 95% CI 3-179). Local drainage, setons, and temporary stoma for deep and complicated fistulas in Crohn's disease, followed by a rectal advancement flap, may result in closing of the stoma in 47% of the time. The risk of permanent fecal diversion was substantial in patients with complicated perianal Crohn's disease, with patients requiring a colorectal resection or suffering from fecal incontinence carrying a particularly high risk for permanent fecal diversion. In contrast, patients with perianal Crohn's disease who required surgery for small bowel disease or a segmental colon resection carried no risk of a permanent stoma.
Figures
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '12996536', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/12996536/'}]}
- Crohn BB, Ginzburg L, Oppenheimer GD. Regional ileitis: A pathologic and clinical entity. JAMA 1932;99:1323–1329. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '1089084', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/1089084/'}]}
- Price AB, Morson BC. The surgical pathology of Crohn’s disease and ulcerative colitis. Human Pathol 1975;6:7–29. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '5909902', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/5909902/'}]}
- Johnson OA, Hoskins DW, Todd J, Thorbjarnarson B. Crohn’s disease of the stomach. Gastroenterology 1996;50:571–577. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '5698629', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/5698629/'}]}
- Gelfand MD, Krone CL. Dysphagia and esophageal ulceration in Crohn’s disease. Gastroenterology 1968;55:510–514. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PMC', 'value': 'PMC1815449', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC1815449/'}, {'type': 'PubMed', 'value': '5363108', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/5363108/'}]}
- Dudeney TP. Crohn’s disease of the mouth. Proc R Soc Med 1969;62:1237. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
