

Review
doi: 10.1086/513442.
Epub 2007 Apr 4.
Genetic factors in congenital diaphragmatic hernia
Affiliations
- PMID: 17436238
- PMCID: PMC1852742
- DOI: 10.1086/513442
Item in Clipboard
Review
Genetic factors in congenital diaphragmatic hernia
Am J Hum Genet.
2007 May.
Abstract
Congenital diaphragmatic hernia (CDH) is a relatively common birth defect associated with high mortality and morbidity. Although the exact etiology of most cases of CDH remains unknown, there is a growing body of evidence that genetic factors play an important role in the development of CDH. In this review, we examine key findings that are likely to form the basis for future research in this field. Specific topics include a short overview of normal and abnormal diaphragm development, a discussion of syndromic forms of CDH, a detailed review of chromosomal regions recurrently altered in CDH, a description of the retinoid hypothesis of CDH, and evidence of the roles of specific genes in the development of CDH.
Figures
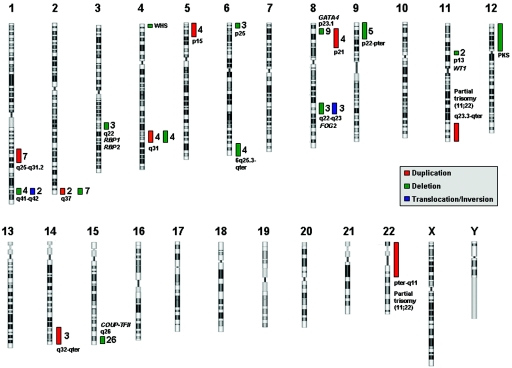
Chromosomal regions and selected candidate genes for CDH. Recurrent chromosomal abnormalities associated with patients with CDH are represented by colored bars. For each region, the number of patients described with that duplication (red bar), deletion (green bar), or translocation/inversion (blue bar) is given. Selected candidate genes and genetic syndromes are included beside their respective regions. PKS = Pallister-Killian syndrome; WHS = Wolf-Hirschorn syndrome.
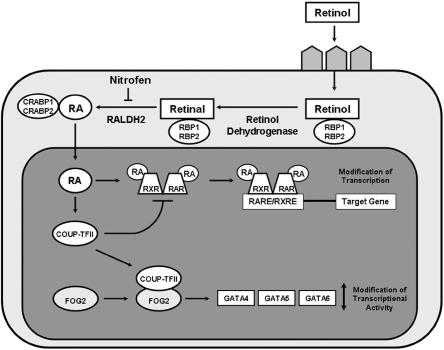
Retinoic acid (RA) signaling pathway and CDH candidate genes. Retinol travels to target cells via the blood and is taken up by receptors on the cell surface. Once in the cytoplasm, retinol is converted to retinal by retinol dehydrogenases and then to RA by retinal dehydrogenases, of which RALDH2 is the predominant enzyme. The action of RALDH2 can be inhibited by teratogens, such as nitrofen. Several binding proteins are present in the cytoplasm, including retinol-binding proteins 1 and 2 (RBP1 and RBP2), which bind retinol and retinal, and cellular RA-binding proteins 1 and 2 (CRABP1 and CRABP2). When RA enters the nucleus, it mediates its effects by binding to RA receptors (RARs) and retinoid X receptors (RXRs). RARs and RXRs dimerize and regulate gene expression by binding to short DNA sequences—RA-responsive elements (RAREs) and retinoid X–responsive elements (RXREs)—located in the vicinity of target genes. COUP-TFII expression is upregulated by RA. COUP-TFII can act as a repressor of this pathway by directly sequestering RXR, thereby preventing heterodimerization to RAR and inhibiting gene transcription. This process may be a negative feedback system that precisely balances the transcription of certain genes during diaphragm development. COUP-TFII has been shown to interact physically with FOG2, which, in turn, modulates the transcriptional activity of GATA4, GATA5, and GATA6.
References
Web Resource
-
- Online Mendelian Inheritance in Man (OMIM), http://www.ncbi.nlm.nih.gov/Omim/ (for CDH, FOG2, GATA4, Fryns syndrome, Beckwith-Wiedemann syndrome, CDKN1C, NDS1, CHARGE syndrome, CHD7, Cornelia de Lange syndrome, NIPBL, SMC1A, craniofrontonasal syndrome, EFNB1, Denys-Drash syndrome, WT1, Donnai-Barrow syndrome, Palister-Killian syndrome, Simpson-Golabi-Behmel syndrome, GPC3, CXORF5, thoracoabdominal syndrome, Wolf-Hirschhorn syndrome, BPES, RBP1, RBP2, Frasier syndrome, Meacham syndrome, and STRA6)
References
-
- Edwards JH (1960) The simulation of Mendelism. Acta Genet Stat Med 10:63–70 - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
- Actions
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
