

Is there a sagittal imbalance of the spine in isthmic spondylolisthesis? A correlation study
- PMID: 17437136
- PMCID: PMC2078287
- DOI: 10.1007/s00586-007-0348-4
Is there a sagittal imbalance of the spine in isthmic spondylolisthesis? A correlation study
Abstract
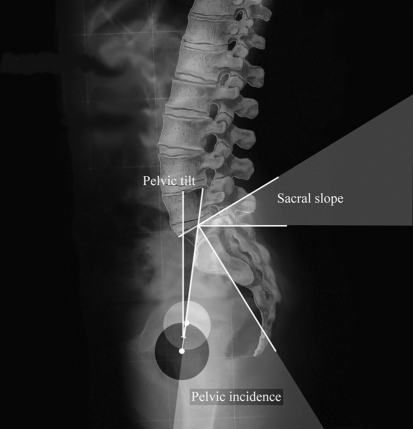
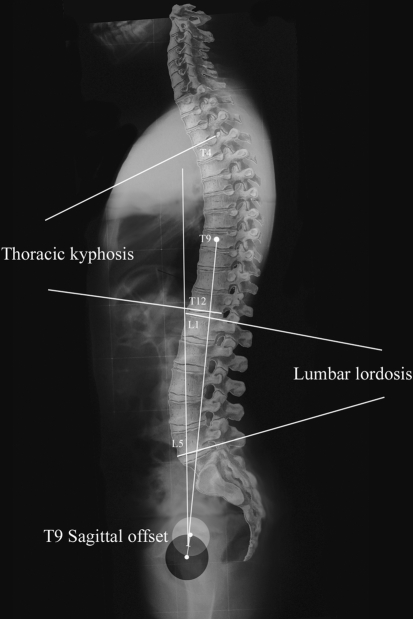
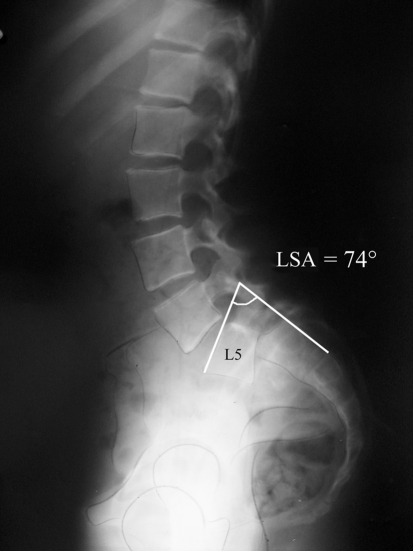
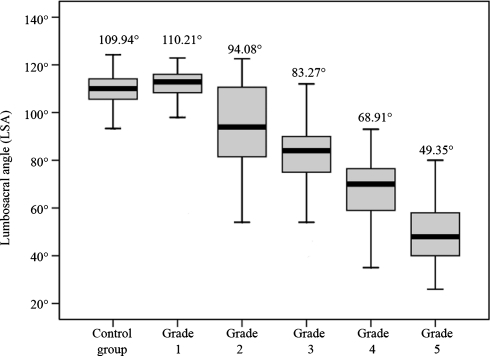
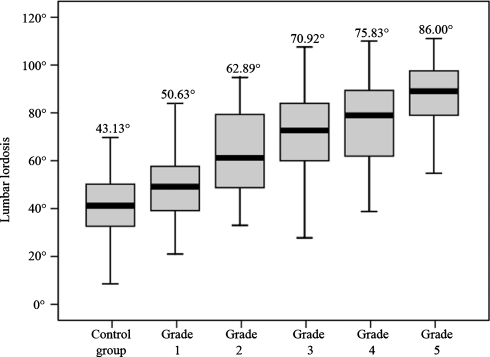
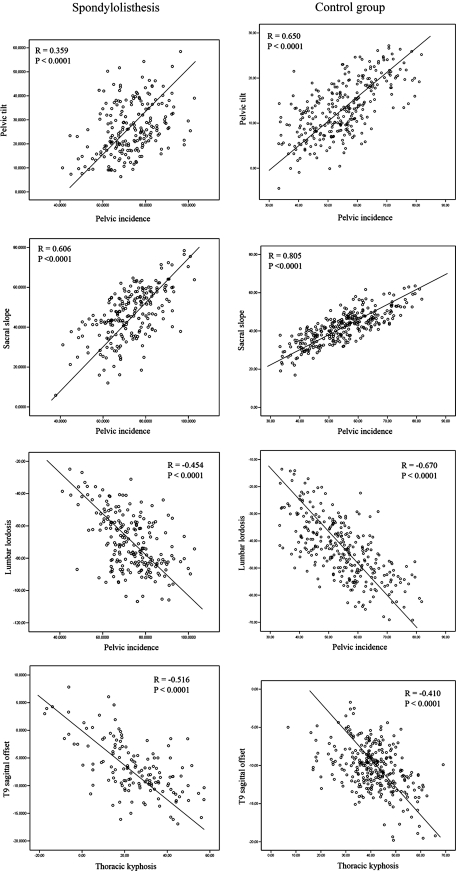
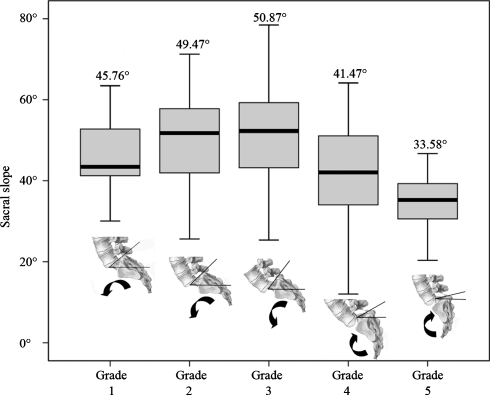
Recent studies suggested a predominant role of spinopelvic parameters to explain lumbosacral spondylolisthesis pathogeny. We compare the pelvic incidence and other parameters of sagittal spinopelvic balance in adolescents and young adults with developmental spondylolisthesis to those parameters in a control group of healthy volunteers. We compared the angular parameters of the sagittal balance of the spine in a cohort of 244 patients with a developmental L5-S1 spondylolisthesis with those of a control cohort of 300 healthy volunteers. A descriptive and correlation study was performed. The L5 anterior slipping and lumbosacral kyphosis in spondylolisthesis patients was described using multiple regression analysis study. Our study demonstrates that the related measures of sagittal spinopelvic alignment are disturbed in adolescents and young adults with developmental spondylolisthesis. These subjects stand with an increased sacral slope, pelvic tilt and lumbar lordosis but with a decreased thoracic kyphosis. Pelvic incidence was significantly higher in spondylolisthesis patients as compared with controls but was not clearly correlated with the grade of slipping. We showed the same "sagittal balance strategy" in spondylolisthesis patients as in the control group regarding correlations between pelvic incidence, sacral slope, pelvic tilt and lumbar lordosis. We believe that the lumbosacral kyphosis is a stronger factor than pelvic incidence which need to be taken into account as a predominant factor in theories of pathogenesis of lumbosacral spondylolithesis. We thus believe that increased lumbar lordosis associated with L5-S1 spondylolisthesis is secondary to the high pelvic incidence and is an important factor causing high shear stresses at the L5-S1 pars interarticularis. However, the "local" sagittal imbalance of the lumbosacral junction is compensated by adjacent mobile segments in the upper lumbar spine, the pelvis orientation and the thoracic spine. The result is not optimal but a satisfactory global sagittal balance of the trunk, even in the most severe grade of slipping.
Figures
References
-
- Boxall D, Bradford DS, Winter RB, Moe JH. Management of severe spondylolisthesis in children and adolescents. J Bone Joint Surg Am. 1979;61:479–495. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
