

Chlamydia and gonorrhoea in pregnant Batswana women: time to discard the syndromic approach?
- PMID: 17437632
- PMCID: PMC1955709
- DOI: 10.1186/1471-2334-7-27
Chlamydia and gonorrhoea in pregnant Batswana women: time to discard the syndromic approach?
Abstract
Background: Chlamydia and gonorrhoea are major causes of morbidity among women in developing countries. Both infections have been associated with pregnancy-related complications, and case detection and treatment in pregnancy is essential. In countries without laboratory support, the diagnosis and treatment of cervical infections is based on the syndromic approach. In this study we measured the prevalence of chlamydia and gonorrhoea among antenatal care attendees in Botswana. We evaluated the syndromic approach for the detection of cervical infections in pregnancy, and determined if risk scores could improve the diagnostic accuracy.
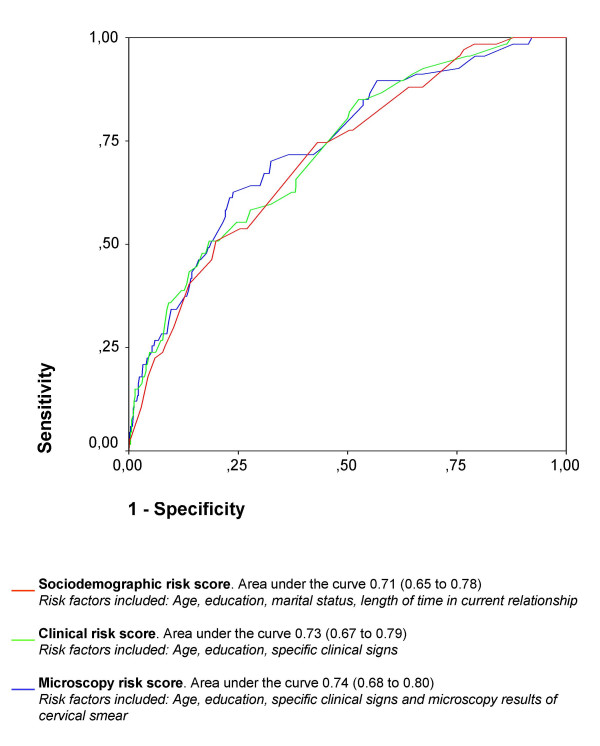
Methods: In a cross-sectional study, 703 antenatal care attendees in Botswana were interviewed and examined, and specimens were collected for the identification of C trachomatis, N gonorrhoeae and other reproductive tract infections. Risk scores to identify attendees with cervical infections were computed based on identified risk factors, and their sensitivities, specificities, likelihood ratios and predictive values were calculated.
Results: The prevalence of chlamydia was 8%, and gonorrhoea was found in 3% of the attendees. Symptoms and signs of vaginal discharge did not predict cervical infection, and a syndromic approach failed to identify infected women. Age (youth) risk factor most strongly associated with cervical infection. A risk score with only sociodemographic factors had likelihood ratios equivalent to risk scores which incorporated clinical signs and microscopy results. However, all the evaluated risk scores were of limited value in the diagnosis of chlamydia and gonorrhoea. A cut-off set at an acceptable sensitivity to avoid infected antenatal care attendees who remained untreated would inevitably lead to considerable over-treatment.
Conclusion: Although in extensive use, the syndromic approach is unsuitable for diagnosing cervical infections in antenatal care attendees in Botswana. None of the evaluated risk scores can replace this management. Without diagnostic tests, there are no adequate management strategies for C trachomatis and N gonorrhoeae in pregnant women in Botswana, a situation which is likely to apply to other countries in sub-Saharan Africa. Screening for cervical infections in pregnant women is an essential public health measure, and rapid tests will hopefully be available in developing countries within a few years.
Figures
Similar articles
-
Risk scores to detect cervical infections in urban antenatal clinic attenders in Mwanza, Tanzania.Sex Transm Infect. 1998 Jun;74 Suppl 1:S139-46. Sex Transm Infect. 1998. PMID: 10023365
-
Risk assessment and other screening options for gonorrhoea and chlamydial infections in women attending rural Tanzanian antenatal clinics.Bull World Health Organ. 1995;73(5):621-30. Bull World Health Organ. 1995. PMID: 8846488 Free PMC article.
-
Prevalence and risk factors for Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis infection in pregnant women in Papua New Guinea.Sex Transm Infect. 2015 May;91(3):194-200. doi: 10.1136/sextrans-2014-051670. Epub 2014 Oct 13. Sex Transm Infect. 2015. PMID: 25313204
-
Lower genital tract infections among pregnant women: a review.East Afr Med J. 2001 Nov;78(11):581-5. East Afr Med J. 2001. PMID: 12219963 Review.
-
Genital Chlamydia trachomatis and Neisseria gonorrhoeae infections among women in sub-Saharan Africa: A structured review.Int J STD AIDS. 2018 Jul;29(8):806-824. doi: 10.1177/0956462418758224. Epub 2018 Feb 28. Int J STD AIDS. 2018. PMID: 29486628 Review.
Cited by
-
Genital Chlamydia trachomatis Infection among Women of Reproductive Age Attending the Gynecology Clinic of Hawassa University Referral Hospital, Southern Ethiopia.PLoS One. 2016 Dec 22;11(12):e0168580. doi: 10.1371/journal.pone.0168580. eCollection 2016. PLoS One. 2016. PMID: 28006003 Free PMC article.
-
Lost opportunity to save newborn lives: variable national antenatal screening policies for Neisseria gonorrhoeae and Chlamydia trachomatis.Int J STD AIDS. 2017 Jun;28(7):660-666. doi: 10.1177/0956462416660483. Epub 2016 Jul 20. Int J STD AIDS. 2017. PMID: 27440873 Free PMC article.
-
Evaluation of Cortez OneStep Chlamydia Rapicard™ Insta Test for the Detection of Chlamydia trachomatis in Pregnant Women at Mbare Polyclinic in Harare, Zimbabwe.Int J MCH AIDS. 2017;6(1):19-26. doi: 10.21106/ijma.150. Int J MCH AIDS. 2017. PMID: 28798890 Free PMC article.
-
The Performance of the Vaginal Discharge Syndromic Management in Treating Vaginal and Cervical Infection: A Systematic Review and Meta-Analysis.PLoS One. 2016 Oct 5;11(10):e0163365. doi: 10.1371/journal.pone.0163365. eCollection 2016. PLoS One. 2016. PMID: 27706174 Free PMC article.
-
Reproductive tract infections in women seeking abortion in Vietnam.BMC Womens Health. 2009 Jan 29;9:1. doi: 10.1186/1472-6874-9-1. BMC Womens Health. 2009. PMID: 19178703 Free PMC article.
References
-
- Over M, Piot P. HIV infection and sexually transmitted diseases. In: Jamison DT, Mosley WH, Measham AR, Bobadilla JS, editor. Disease control priorities in developing countries. Oxford University Press; 1993. pp. 455–527.
-
- UNAIDS/WHO Consultation on STD interventions forpreventing HIV: what is the evidence? Geneva. 2000. http://www.who.int/hiv/pub/sti/pubevidence/en/
-
- WHO Guidelines for the management of sexually transmitted infections Geneva. 2003. http://whqlibdoc.who.int/publications/2003/9241546263.pdf
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
