

Antibody to aquaporin 4 in the diagnosis of neuromyelitis optica
- PMID: 17439296
- PMCID: PMC1852124
- DOI: 10.1371/journal.pmed.0040133
Antibody to aquaporin 4 in the diagnosis of neuromyelitis optica
Abstract
Background: Neuromyelitis optica (NMO) is a demyelinating disease of the central nervous system (CNS) of putative autoimmune aetiology. Early discrimination between multiple sclerosis (MS) and NMO is important, as optimum treatment for both diseases may differ considerably. Recently, using indirect immunofluorescence analysis, a new serum autoantibody (NMO-IgG) has been detected in NMO patients. The binding sites of this autoantibody were reported to colocalize with aquaporin 4 (AQP4) water channels. Thus we hypothesized that AQP4 antibodies in fact characterize NMO patients.
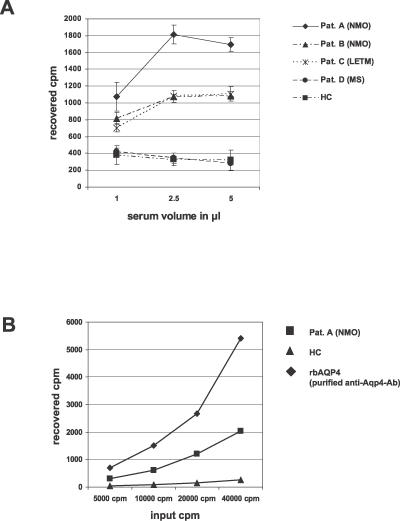
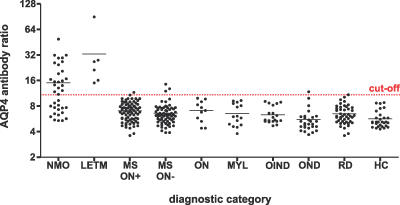
Methods and findings: Based on these observations we cloned human water channel AQP4, expressed the protein in a eukaryotic transcription/translation system, and employed the recombinant AQP4 to establish a new radioimmunoprecipitation assay (RIPA). Indeed, application of this RIPA showed that antibodies against AQP4 exist in the majority of patients with NMO (n = 37; 21 positive) as well as in patients with isolated longitudinally extensive transverse myelitis (n = 6; six positive), corresponding to a sensitivity of 62.8% and a specificity of 98.3%. By contrast, AQP4 antibodies were virtually absent in 291 other participants, which included patients with MS (n = 144; four positive), patients with other inflammatory and noninflammatory neurological diseases (n = 73; one positive), patients with systemic autoimmune diseases (n = 45; 0 positive), and healthy participants (n = 29; 0 positive).
Conclusions: In the largest series reported so far to our knowledge, we quantified AQP4 antibodies in patients with NMO versus various other diseases, and showed that the aquaporin 4 water channel is a target antigen in a majority of patients with NMO. The newly developed assay represents a highly specific, observer-independent, and easily reproducible detection method facilitating clinically relevant discrimination between NMO, MS, and other inflammatory diseases.
Conflict of interest statement
Figures
References
-
- Wingerchuk DM, Hogancamp WF, O'Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic's syndrome) Neurology. 1999;53:1107–1114. - PubMed
-
- Wingerchuk DM, Weinshenker BG. Neuromyelitis optica: Clinical predictors of a relapsing course and survival. Neurology. 2003;60:848–853. - PubMed
-
- Cree BA, Goodin DS, Hauser SL. Neuromyelitis optica. Semin Neurol. 2002;22:105–122. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
