

Cost-effectiveness of preventative therapies for postmenopausal women with osteopenia
- PMID: 17439652
- PMCID: PMC1866224
- DOI: 10.1186/1472-6874-7-6
Cost-effectiveness of preventative therapies for postmenopausal women with osteopenia
Abstract
Background: Limited data are available regarding the cost-effectiveness of preventative therapies for postmenopausal women with osteopenia. The objective of the present study was to evaluate the cost-effectiveness of raloxifene, alendronate and conservative care in this population.
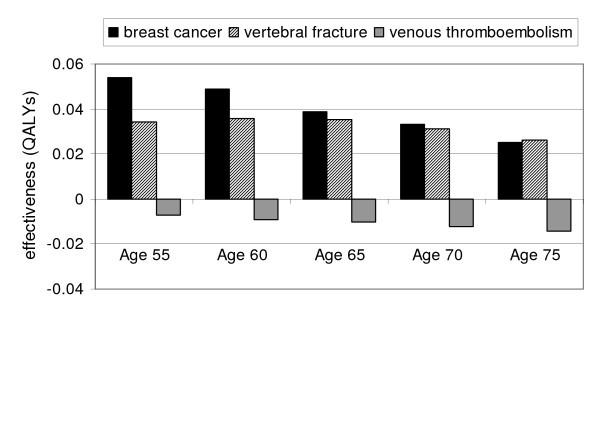
Methods: We developed a microsimulation model to assess the incremental cost and effectiveness of raloxifene and alendronate relative to conservative care. We assumed a societal perspective and a lifetime time horizon. We examined clinical scenarios involving postmenopausal women from 55 to 75 years of age with bone mineral density T-scores ranging from -1.0 to -2.4. Modeled health events included vertebral and nonvertebral fractures, invasive breast cancer, and venous thromboembolism (VTE). Raloxifene and alendronate were assumed to reduce the incidence of vertebral but not nonvertebral fractures; raloxifene was assumed to decrease the incidence of breast cancer and increase the incidence of VTEs. Cost-effectiveness is reported in $/QALYs gained.
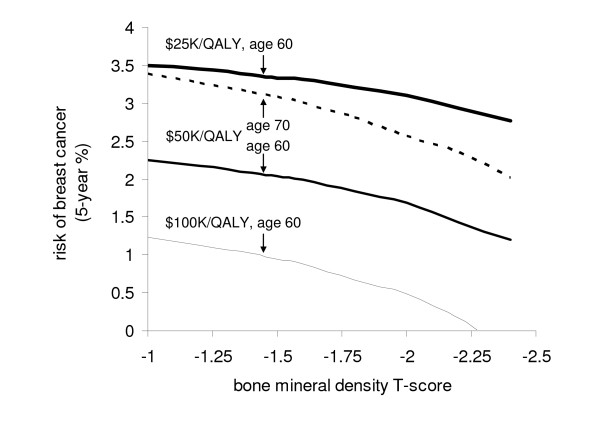
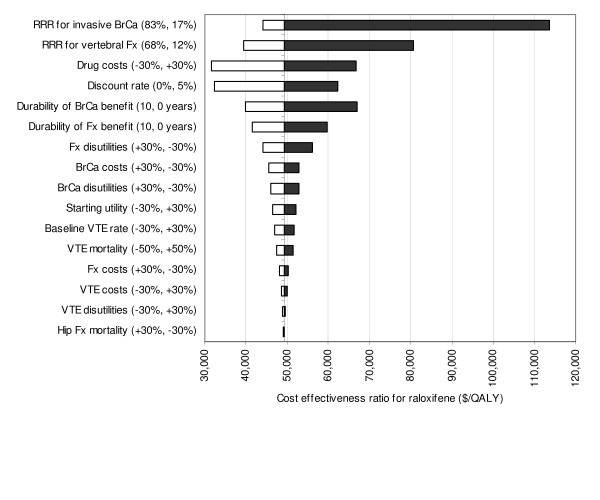
Results: For women 55 to 60 years of age with a T-score of -1.8, raloxifene cost approximately $50,000/QALY gained relative to conservative care. Raloxifene was less cost-effective for women 65 and older. At all ages, alendronate was both more expensive and less effective than raloxifene. In most clinical scenarios, raloxifene conferred a greater benefit (in QALYs) from prevention of invasive breast cancer than from fracture prevention. Results were most sensitive to the population's underlying risk of fracture and breast cancer, assumed efficacy and costs of treatment, and the discount rate.
Conclusion: For 55 and 60 year old women with osteopenia, treatment with raloxifene compares favorably to interventions accepted as cost-effective.
Figures
References
-
- World Health Organization (WHO Study Group) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: report of a WHO Study Group. World Health Organ Tech Rep Ser. 1994;843:1–129. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
