

Irritable bowel syndrome and negative appendectomy: a prospective multivariable investigation
- PMID: 17440183
- PMCID: PMC1942162
- DOI: 10.1136/gut.2006.112672
Irritable bowel syndrome and negative appendectomy: a prospective multivariable investigation
Abstract
Objective: To examine prospectively whether irritable bowel syndrome (IBS) or other variables-that is, psychiatric profiles, health-related quality of life (HRQoL) and clinical features-are associated with negative appendectomy (NA).
Design: Longitudinal study.
Setting: Inpatient and emergency service in a university-affiliated teaching hospital.
Patients: 430 consecutive patients underwent emergent surgery for suspected appendicitis.
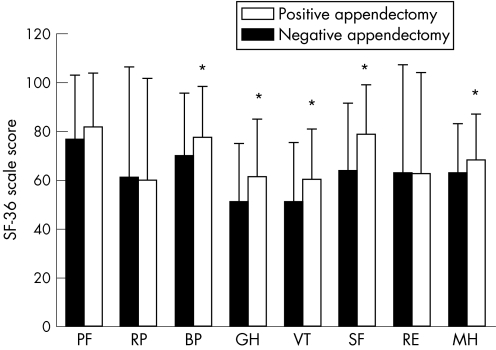
Main outcome measures: Rome-II IBS questionnaire; the Hospital Anxiety and Depression Scale; the Short-Form 36 survey; the clinical, pathological and CT findings.
Results: The NA group (n = 68, 15.8%) was younger, with female predominance, higher prevalence of Rome-II IBS, higher anxiety/depression scores and lower levels of HRQoL than the positive appendectomy group. The patients with NA tended to have atypical presentations (absence of migration pain/fever/muscle guarding), lower white cell count and percentage of polymorphonuclear cells (PMNC) and lower rate of CT scan usage than the positive group. After multiple logistic regression, IBS (OR 2.17; 95% CI 1.14 to 4.24), degree of anxiety (OR 1.12; 95% CI 1.02 to 1.49), absence of migrating pain (OR 3.43; 95% CI 1.90 to 5.95)/muscle guarding (OR 3.72; 95% CI 2.07 to 6.70), a lower PMNC percentage (<75%; OR 3.05; 95% CI 1.69 to 5.51) and no CT scan usage (OR 2.32; 95% CI 1.27 to 4.26) were found to be the independent factors in predicting NA.
Conclusion: Both patient (IBS, anxiety, atypical presentation) and physician (low CT scan usage) factors are the independent determinants predicting NA. Physicians should be cautious before operating on or referring patients with IBS for appendectomy. CT scan should be considered in patients with suspected appendicitis, particularly in those with IBS and atypical clinical presentations.
Conflict of interest statement
Competing interests: None.
Comment in
-
Avoiding unnecessary surgery in irritable bowel syndrome.Gut. 2007 May;56(5):608-10. doi: 10.1136/gut.2006.115006. Gut. 2007. PMID: 17440179 Free PMC article.
-
Irritable bowel syndrome and negative appendectomy.Gut. 2007 Oct;56(10):1479. Gut. 2007. PMID: 17872582 Free PMC article. No abstract available.
References
-
- Flum D R, Koepsell T. The clinical and economic correlates of misdiagnosed appendicitis: nationwide analysis. Arch Surg 2002137799–804. - PubMed
-
- Addiss D G, Shaffer N, Fowler B S.et al The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol 1990132910–925. - PubMed
-
- Korner H, Sondenaa K, Soreide J A.et al Incidence of acute nonperforated and perforated appendicitis: age‐specific and sex‐specific analysis. World J Surg 199721313–317. - PubMed
-
- Pittman‐Waller V A, Myers J G, Stewart R M.et al Appendicitis: why so complicated? Analysis of 5755 consecutive appendectomies. Am Surg 200066548–554. - PubMed
-
- Flum D R, Morris A, Koepsell T.et al Has misdiagnosis of appendicitis decreased over time? A population‐based analysis. JAMA 20012861748–1753. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical