

Safety and efficacy of a caspofungin-based combination therapy for treatment of proven or probable aspergillosis in pediatric hematological patients
- PMID: 17442100
- PMCID: PMC1871594
- DOI: 10.1186/1471-2334-7-28
Safety and efficacy of a caspofungin-based combination therapy for treatment of proven or probable aspergillosis in pediatric hematological patients
Abstract
Background: Fungal infections are diagnosed increasingly often in patients affected by hematological diseases and their mortality has remained high. The recent development of new antifungal drugs gives the clinician the possibility to assess the combination of antifungal drugs with in-vitro or in animal-model synergistic effect.
Methods: We analyzed retrospectively the safety and efficacy of caspofungin-based combination therapy in 40 children and adolescents, most of them were being treated for a malignant disease, who developed invasive aspergillosis (IA) between November 2002 and November 2005.
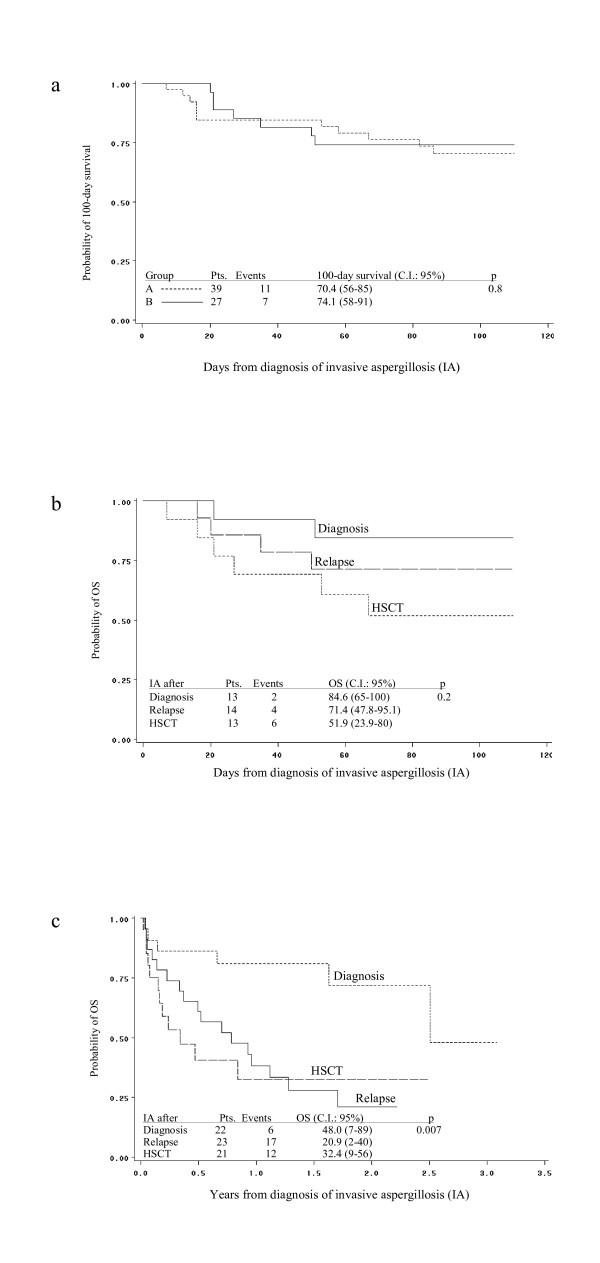
Results: Thirteen (32.5%) patients developed IA after hematopoietic stem cell transplantation (HSCT), 13 after primary diagnosis, usually during remission-induction chemotherapy, and 14 after relapse of disease. Severe neutropenia was present in 31 (78%) out of the 40 patients. IA was classified as probable in 20 (50%) and documented in 20 (50%) patients, respectively. A favorable response to antifungal therapy was obtained in 21 patients (53%) and the probability of 100-day survival was 70%. Different, though not significant, 100-day survival was observed according to the timing of diagnosis of IA: 51.9% after HSCT; 71.4% after relapse; and 84.6% after diagnosis of underlying disease, p 0.2. After a median follow-up of 0.7 years, 20 patients are alive (50%). Overall, the combination therapy was well tolerated. In multivariate analysis, the factors that were significantly associated to a better overall survival were favorable response to antifungal therapy, p 0.003, and the timing of IA in the patient course of underlying disease, p 0.04.
Conclusion: This study showed that caspofungin-based combination antifungal therapy is an effective therapeutic option also for pediatric patients with IA. These data need to be confirmed by prospective, controlled studies.
Figures
References
-
- Morgan J, Wannemuehler KA, Marr KA, Hadley S, Kontoyiannis DP, Walsh TJ, Fridkin SK, Pappas PG, Warnock DW. Incidence of invasive aspergillosis following hematopoietic stem cell and solid organ transplantation: interim results of a prospective multicenter surveillance program. Med Mycol. 2005;43:S49–S58. doi: 10.1080/13693780400020113. - DOI - PubMed
-
- Herbrecht R, Denning DW, Patterson TF, Bennett JE, Greene RE, Oestmann JW, Kern WV, Marr KA, Ribaud P, Lortholary O, Sylvester R, Rubin RH, Wingard JR, Stark P, Durand C, Caillot D, Thiel E, Chandrasekar PH, Hodges MR, Schlamm HT, Troke PF, de Pauw B, Invasive Fungal Infections Group of the European Organisation for Research and Treatment of Cancer and the Global Aspergillus Study Group Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. N Engl J Med. 2002;347:408–415. doi: 10.1056/NEJMoa020191. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
