

Total hip arthroplasties: what are the reasons for revision?
- PMID: 17443324
- PMCID: PMC2551710
- DOI: 10.1007/s00264-007-0364-3
Total hip arthroplasties: what are the reasons for revision?
Abstract
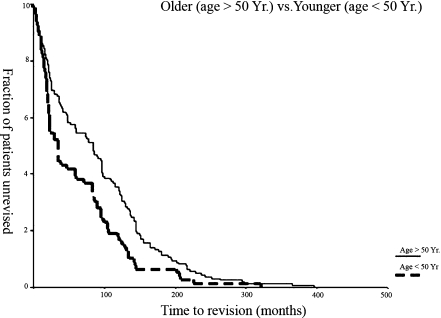
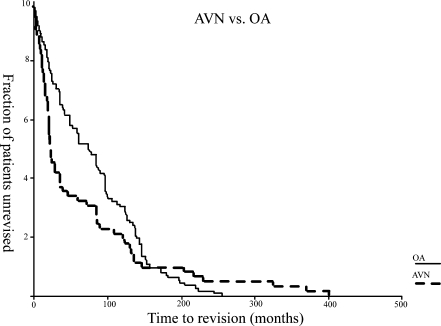
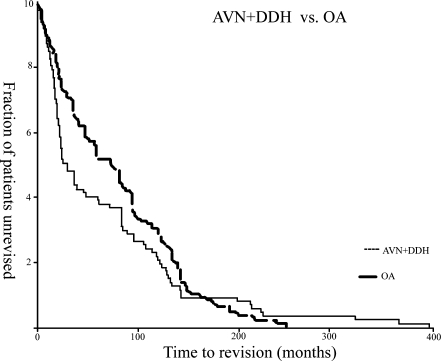
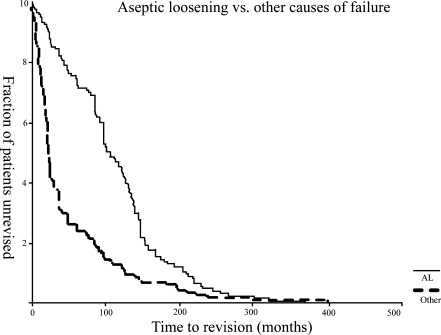
Primary total hip arthroplasties have reported success rates of greater than 95% in many series with a longer than 10-year follow-up. Revision total hip arthroplasty due to such factors as increased high-activity levels, younger patients undergoing the procedure and increasing life expectancy has become more prevalent. An understanding of the mechanisms and timing of total hip arthroplasty failure can direct efforts aimed at reducing revision rates. This study was conducted to evaluate the indications for revision hip arthroplasty and relate these to the time after the index primary hip arthroplasty. A review of all revision hip arthroplasties at two centres over a 6-year time period identified 225 patients who underwent 237 revisions. The overall mean time to revision was 83 months (range: 0-360 months). The cause of failure was aseptic loosening in 123 hips (51.9%), instability in 40 hips (16.9%) and infection in 37 hips (5.5%). When stratified into two groups (less than 5 years, more than 5 years after the index primary hip arthroplasty), 118 of 237 (50%) revisions occurred in less than 5 years, with 33% due to instability and 24% resulting from infection. The majority of the causes of failure within 5 years in these early revisions were instability and deep infection. The success of hip arthroplasty is likely to be compromized if technical aspects of the surgery for appropriate component positioning and critical protocols to minimise complications such as infection are not given the proper attention.
A dix ans de recul moyen les prothèses totales de hanches ont un taux de 95% de réussite dans la plupart des séries. Les facteurs ayant entraînés une réintervention, de type révision dépendent du niveau d’activité des sujets, de leurs jeunes âges, et de l’augmentation de la durée de vie. La compréhension des mécanismes d’échecs des prothèses totales de hanche devrait permettre de réduire le taux de révision. Cette étude a pour but d’évaluer les indications de révisions des prothèses totales de hanche. Pour cela, ont été revus, dans deux centres, avec six ans de recul moyen 225 patients qui ont bénéficié de 237 révisions. Le temps moyen pour la révision a été de 83 mois (0 à 360 mois). La cause de l’échec a été le descellement aseptique 123 hanches (51.9%), instabilité sur 40 hanches (16.9%) et infection sur 37 hanches (5.5%). Si l’on reclasse ces patients en deux groupes à moins et plus de 5 ans, 118 des 237 révisions (50%) surviennent dans une période de moins de 5 ans, 33% sont dues à l’instabilité, 24% à l’infection. Les causes d’échecs majeures avant 5 ans avec révisions, sont donc l’instabilité de la hanche et les infections profondes. Le succès d’une arthroplastie totale de hanche passe donc par le bon positionnement des implants et le respect du protocole de façon à éviter les complications infectieuses.
Figures
References
-
- Mahomed NN, Barrett JA, Katz JN, et al. Rates and outcomes of primary and revision total hip replacement in the United States medicare population. J Bone Jnt Surg Am. 2003;85-A(1):27–32. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
