

Group visits: promoting adherence to diabetes guidelines
- PMID: 17443369
- PMCID: PMC1852919
- DOI: 10.1007/s11606-007-0150-3
Group visits: promoting adherence to diabetes guidelines
Abstract
Background: Current diabetes management guidelines offer blueprints for providers, yet type 2 diabetes control is often poor in disadvantaged populations. The group visit is a new treatment modality originating in managed care for efficient service delivery to patients with chronic health problems. Group visits offer promise for delivering care to diabetic patients, as visits are lengthier and can be more frequent, more organized, and more educational.
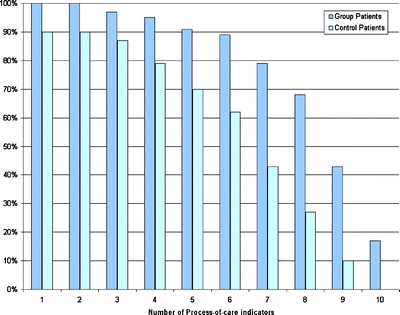
Objective: To evaluate the effect of group visits on clinical outcomes, concordance with 10 American Diabetes Association (ADA) guidelines [American Diabetes Association, Diabetes Care, 28:S4-36, 2004] and 3 United States Preventive Services Task Force (USPSTF) cancer screens [U.S. Preventive Services Task Force, http://www.ahrq.gov/clinic/uspstf/resource.htm, 2003].
Research design and methods: A 12-month randomized controlled trial of 186 diabetic patients comparing care in group visits with care in the traditional patient-physician dyad. Clinical outcomes (HbA1c, blood pressure [BP], lipid profiles) were assessed at 6 and 12 months and quality of care measures (adherence to 10 ADA guidelines and 3 USPSTF cancer screens) at 12 months.
Results: At both measurement points, HbA1c, BP, and lipid levels did not differ significantly for patients attending group visits versus those in usual care. At 12 months, however, patients receiving care in group visits exhibited greater concordance with ADA process-of-care indicators (p < .0001) and higher screening rates for cancers of the breast (80 vs. 68%, p = .006) and cervix (80 vs 68%, p = .019).
Conclusions: Group visits can improve the quality of care for diabetic patients, but modifications to the content and style of group visits may be necessary to achieve improved clinical outcomes.
Figures
References
-
- Centers for Disease Control and Prevention. National diabetes fact sheet, United States, 2003. Atlanta, GA, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; 2003.
-
- Beck A, Scott J, Williams C, et al. Cooperative health care clinics: a group approach to individual care. JAGS. 1997;45:543–9.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
