

Prolonged versus short course of indomethacin for the treatment of patent ductus arteriosus in preterm infants
- PMID: 17443527
- PMCID: PMC8715534
- DOI: 10.1002/14651858.CD003480.pub3
Prolonged versus short course of indomethacin for the treatment of patent ductus arteriosus in preterm infants
Abstract
Background: Indomethacin is a prostaglandin inhibitor used to treat patent ductus arteriosus (PDA) in preterm infants. Although indomethacin produces ductal closure in the majority of cases, it is ineffective in up to 40% of patients. Furthermore, the ductus will re-open in up to 35% of infants who initially respond to the drug. Prolonging the course of indomethacin has the potential to achieve higher rates of ductal closure.
Objectives: To determine the effect of a prolonged course of indomethacin (compared to a short course) on the rate of treatment failure without unwanted side-effects in preterm infants with PDA.
Search strategy: The search included review of personal files, abstracts of conferences, and the following electronic databases: MEDLINE (1966 to December 2006), EMBASE (1974 to December 2006), and Oxford Database of Perinatal Trials, Cochrane Central Register of Controlled Trials (The Cochrane Library, Issue 4, 2006). No language restrictions were applied.
Selection criteria: Randomized or quasi-randomized controlled trials including preterm infants with PDA, diagnosed on clinical and/or echocardiographic examination that evaluated indomethacin treatment by any route given as a long course (four or more doses) vs. a short course (three or fewer doses) were included in the review. Trials needed to report on at least one of the following outcomes: failure of PDA to close, need for re-treatment, PDA re-opening, PDA ligation, mortality, duration of assisted ventilation, chronic lung disease (CLD), duration of supplemental oxygen dependence, intraventricular hemorrhage (IVH) (all and severe), diminished urine output, increased serum creatinine, necrotizing enterocolitis (NEC), bleeding diathesis, retinopathy of prematurity (ROP), and duration of hospital stay.
Data collection and analysis: The three review authors independently abstracted data from each study. Relative risk (RR) and Risk Difference (RD) with 95% confidence intervals (CI) using the fixed effect model for meta-analysis are reported. When a statistically significant RD was found, the number needed to treat (NNT) or number needed to harm (NNH) was also calculated with 95% CIs. The I squared statistic was used to test for heterogeneity of results among included trials.
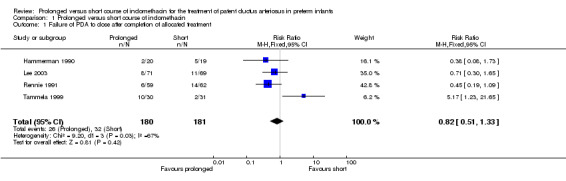
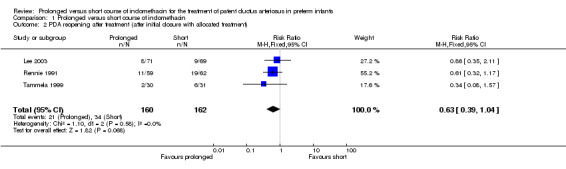
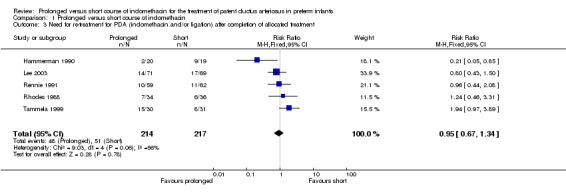
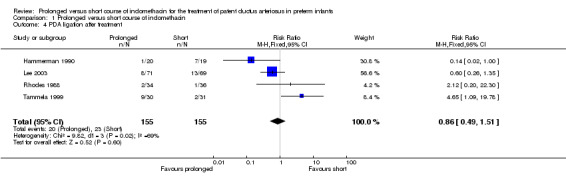
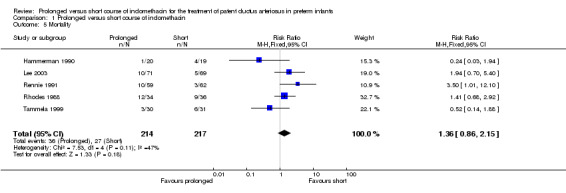
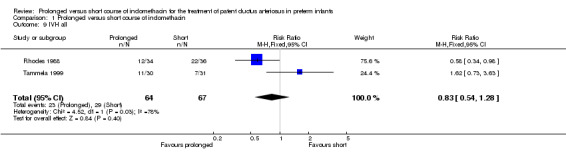
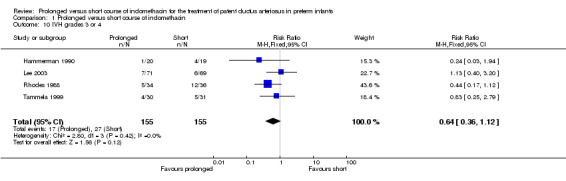
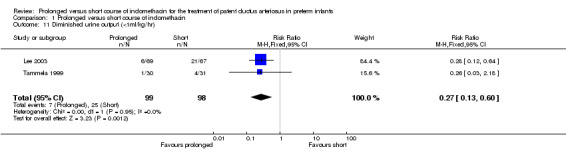
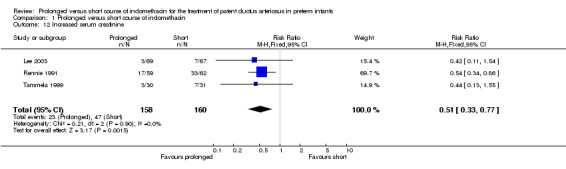
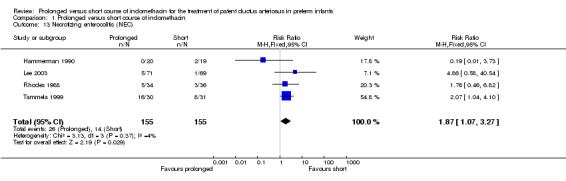
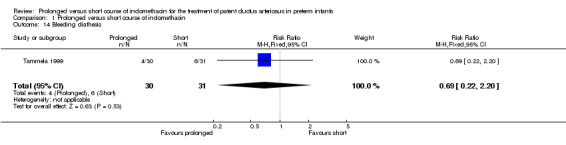
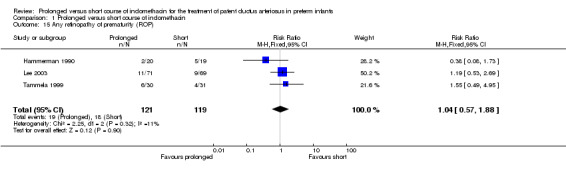
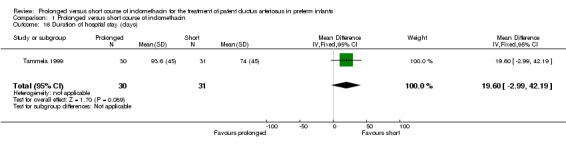
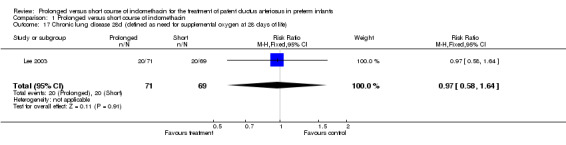
Main results: Five trials met inclusion criteria and included 431 infants. Prolonged indomethacin treatment when compared to the short course did not result in a statistically significant difference in PDA closure, re-treatment, re-opening, or ligation rates. The prolonged course was associated with an increased risk of NEC [typical RR 1.87 (95% CI 1.07, 3.27); typical RD 0.08 (95% CI 0.01, 0.15); NNH 13 (7, 100)] and a decreased incidence of renal function impairment, as evidenced by a lower proportion of infants having diminished urine output [typical RR 0.27 (95% CI 0.13, 0.6); typical RD -0.19 (95% CI -0.28, -0.09); NNT 5 (4, 11)] and increased serum creatinine level [typical RR 0.51 (95% CI 0.33, 0.77); typical RD -0.14 (95% CI -0.23, -0.06); NNT 7 (4, 16)].
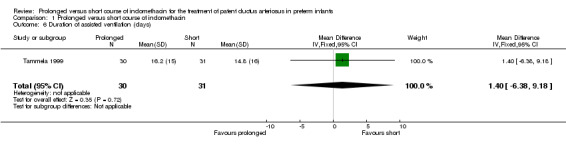
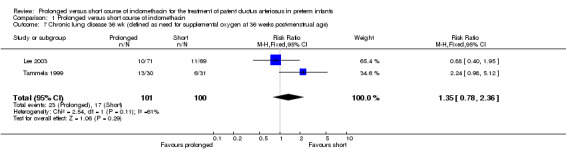
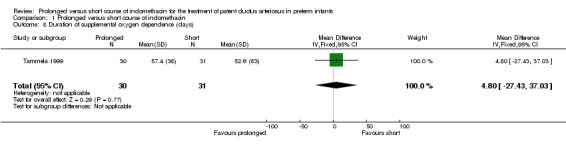
Authors' conclusions: Implications for practiceProlonged indomethacin course does not appear to have a significant effect on improving important outcomes, such as PDA treatment failure, CLD, IVH, or mortality. The reduction of transient renal impairment does not outweigh the increased risk of NEC associated with the prolonged course. Based on these results, a prolonged course of indomethacin cannot be recommended for the routine treatment of PDA in preterm infants. Implications for researchThere is a paucity of data on optimal dosing and duration of indomethacin therapy for the treatment of PDA, in particular for extremely low birth weight infants (ELBW) premature infants. It is likely that a single standard indomethacin regime is not the ideal for every premature infant. Therefore, individual patient response should be considered and evaluated, in particular in ELBW infants. Future randomized clinical trials should include this high risk population and investigate the effect of tailoring dose and duration of therapy to individual response in terms of echocardiographic findings and/or prostaglandin levels, focusing on clinically significant outcomes, including long-term neurodevelopmental outcomes. In addition, factors that may influence treatment effect, such as birth weight, gestational age, age at the time of randomization, total fluid intake, feeding practice, and severity of PDA, need to be taken into account when designing such studies.
Conflict of interest statement
None
Figures
Update of
-
Prolonged versus short course of indomethacin for the treatment of patent ductus arteriosus in preterm infants.Cochrane Database Syst Rev. 2004;(1):CD003480. doi: 10.1002/14651858.CD003480.pub2. Cochrane Database Syst Rev. 2004. Update in: Cochrane Database Syst Rev. 2007 Apr 18;(2):CD003480. doi: 10.1002/14651858.CD003480.pub3. PMID: 14974018 Updated.
References
References to studies included in this review
Hammerman 1990 {published data only}
-
- Hammerman C, Aramburo MJ. Prolonged indomethacin therapy for the prevention of recurrences of patent ductus arteriosus. Journal of Pediatrics 1990;117:771‐6. - PubMed
Lee 2003 {published data only}
-
- Lee J, Rajadurai VS, Tan KW, Wong KY, Wong EH, Leong JY. Randomized trial of prolonged low‐dose versus conventional‐dose indomethacin for treating patent ductus arteriosus in very low birth weight infants. Pediatrics 2003;112:345‐50. - PubMed
Rennie 1991 {published data only}
Rhodes 1988 {published data only}
-
- Rhodes PG, Ferguson MG, Reddy NS, Joransen JA, Gibson J. Effects of prolonged versus acute indomethacin therapy in very low birth‐weight infants with patent ductus arteriosus. European Journal of Pediatrics 1988;147:481‐4. - PubMed
Tammela 1999 {published data only}
-
- Tammela O, Ojala R, Iivainen T, Lautamatti L, Pokela M, Janas M, et al. Short versus prolonged indomethacin therapy for patent ductus arteriosus in preterm infants. Journal of Pediatrics 1999;134:552‐7. - PubMed
References to studies awaiting assessment
VanOvermeire 2001 {published data only}
-
- Overmeire B, Rienstra M, Groore K. Short versus prolonged indomethacin therapy for retreatment of patent ductus arteriosus in preterm infants. Pediatric Research 2001;49:375 A.
Additional references
Bell 1978
Brook 1995
-
- Brook M, Heymann M. Patent ductus arteriosus. In: Emmanouilides GC, Riemenschneider TA, Allen HD, Gutgesell HP editor(s). Heart Disease in Infants, Children, and Adolescents Including the Fetus and Young Adult. Williams & Wilkins, 1995:746‐4.
Clyman 1996
-
- Clyman RI. Recommendations for the postnatal use of indomethacin: an analysis of four separate treatment strategies. Journal of Pediatrics 1996;128:601‐7. - PubMed
Cotton 1978
-
- Cotton RB, Stahlman MT, Kovar I, Catterton WZ. Medical management of small preterm infants with symptomatic patent ductus arteriousus. Journal of Pediatrics 1978;92:467‐73. - PubMed
Friedman 1976
-
- Friedman WF, Hirschklau MJ, Printz MP, Pitlick PT, Kirkpatrick SE. Pharmacologic closure of patent ductus arteriosus in the premature infant. New England Journal of Medicine 1976;295:526‐9. - PubMed
Gersony 1983
-
- Gersony WM, Peckham GJ, Ellison RC, Miettinen OS, Nadas AS. Effects of indomethacin on premature infants with patent ductus arteriosus: results of a national collaborative study. Journal of Pediatrics 1983;102:895‐906. - PubMed
Hammerman 1995
-
- Hammerman C. Patent ductus arteriosus. Clinical relevance of prostaglandins and prostaglandin inhibitors in PDA pathophysiology and treatment. Clinics in Perinatology 1995;22:457‐79. - PubMed
Heymann 1976
-
- Heymann MA, Rudolph AM, Silverman NH. Closure of the ductus arteriosus in premature infants by inhibition of prostaglandin synthesis. New England Journal of Medicine 1976;295:530‐3. - PubMed
Itabashi 2003
-
- Itabashi K, Ohno T, Nishida H. Indomethacin responsiveness of patent ductus arteriosus and subsequent renal abnormalities in preterm infants treated with indomethacin. Journal of Pediatrics 2003;143:203‐7. - PubMed
Kluckow 2000
-
- Kluckow M, Evans N. Ductal shunting, high pulmonary blood flow and pulmonary hemorrhage. Journal of Pediatrics 2000;137:68‐72. - PubMed
Papile 1978
-
- Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. Journal of Pediatrics 1978;92:529‐34. - PubMed
Qinn 2002
-
- Quinn D, Cooper B, Clyman RI. Factors associated with permanent closure of the ductus arteriosus: a role for prolonged indomethacin therapy. Pediatrics 2002;110:e10. - PubMed
Rojas 1995
-
- Rojas M, Gonzalez A, Bancalari E, Claure N, Poole C, Silva‐Neto G. Changing trends in the epidemiology and pathogenesis of neonatal chronic lung disease. Journal of Pediatrics 1995;126:605‐10. - PubMed
Schmidt 2001
-
- Schmidt B, Davis P, Moddemann D, Ohlsson A, Roberts R, Saigal S, et al. Long‐term effects of indomethacin prophylaxis in extremely‐low‐birth‐weight infants. New England Journal of Medicine 2001;344:1966‐72. - PubMed
Seyberth 1982
-
- Seyberth HW, Muller H, Wille L, Pluckthun H, Wolf D, Ulmer HE. Recovery of prostaglandin production associated with reopening of the ductus arteriosus after indomethacin treatment in preterm infants with respiratory distress syndrome. Pediatric Pharmacology 1982;2:127‐41. - PubMed
Seyberth 1983
-
- Seyberth HW, Knapp G, Wolf D, Ulmer HE. Introduction of plasma indomethacin level monitoring and evaluation of an effective threshold level in very low birth weight infants with symptomatic patent ductus arteriosus. European Journal of Pediatrics 1983;141:71‐6. - PubMed
Shaffer 2002
-
- Shaffer CL, Gal P, Ransom JL, Carlos RQ, Smith MS, Davey AM, Dimaguila MA, Brown YL, Schall SA. Effect of age and birth weight on indomethacin pharmacodynamics in neonates treated for patent ductus arteriosus. Critical Care Medicine 2002;30:343‐8. - PubMed
Siassi 1976
-
- Siassi B, Blanco C, Cabal L, Coran A. Incidence and clinical features of patent ductus arteriosus in low birthweight infants: a prospective analysis of 150 consecutively born infants. Pediatrics 1976;57:347‐51. - PubMed
Sinclair 1992
-
- Sinclair JC, Bracken MB. Effective care of the newborn infant. Oxford, Oxford University Press, 1992.
Walters 1988
Yaffe 1980
-
- Yaffe SJ, Friedman WF, Rogers D, Lang P, Ragni M, Saccar C. The disposition of indomethacin in preterm babies. Journal of Pediatrics 1980;97:1001‐6. - PubMed
Yeh 1983
Yeh 1991
-
- Yeh TF, Carr I. Pharmacologic closure of ductus arteriosus. Drug Therapy in the Neonate and Small Infant. 2nd Edition. Chicago: Year Book, 1991:123‐38.
References to other published versions of this review
Herrera 2004
-
- Herrera C, Holberton J, Davis P. Prolonged versus short course of indomethacin for the treatment of patent ductus arteriosus in preterm infants. Cochrane Database of Systematic Reviews 2004, Issue 1. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous