

Analyses of the 1957 (Asian) influenza pandemic in the United Kingdom and the impact of school closures
- PMID: 17445311
- PMCID: PMC2870798
- DOI: 10.1017/S0950268807008369
Analyses of the 1957 (Asian) influenza pandemic in the United Kingdom and the impact of school closures
Abstract
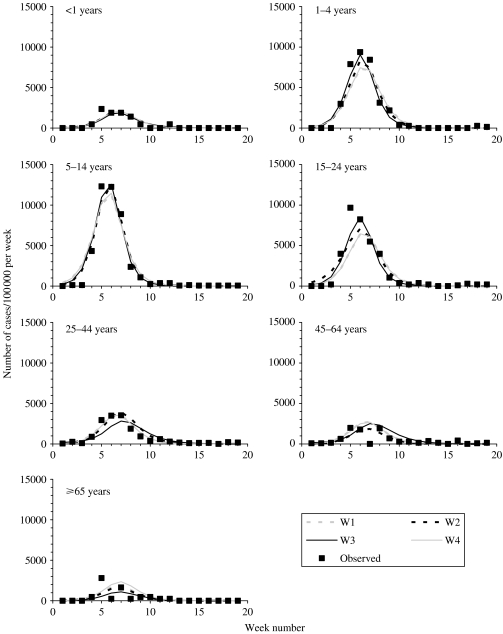
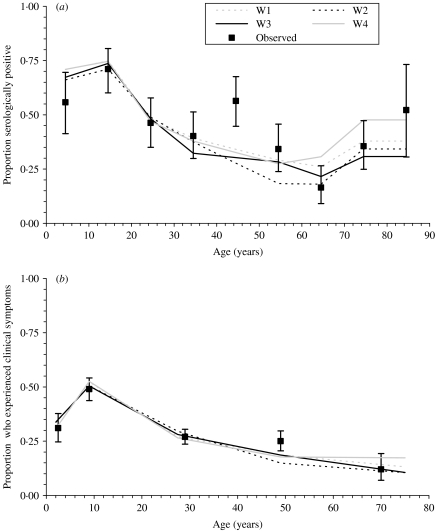
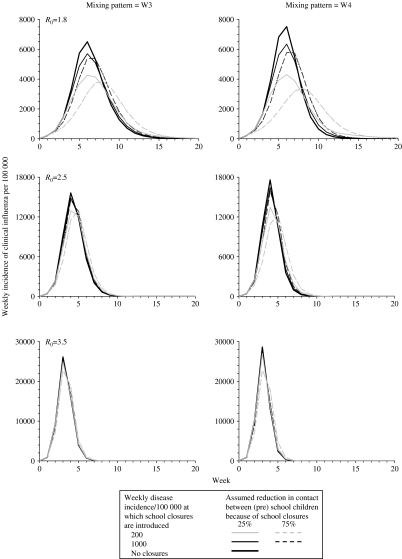
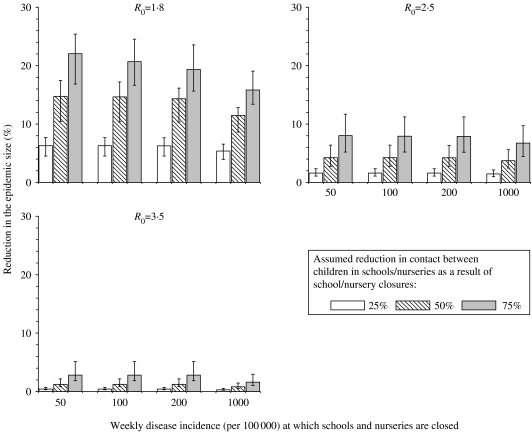
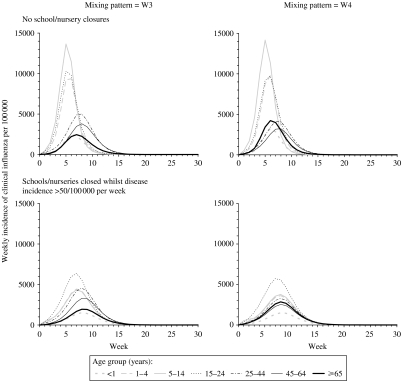
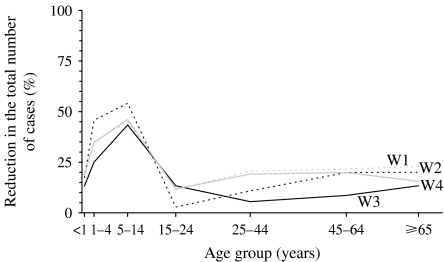
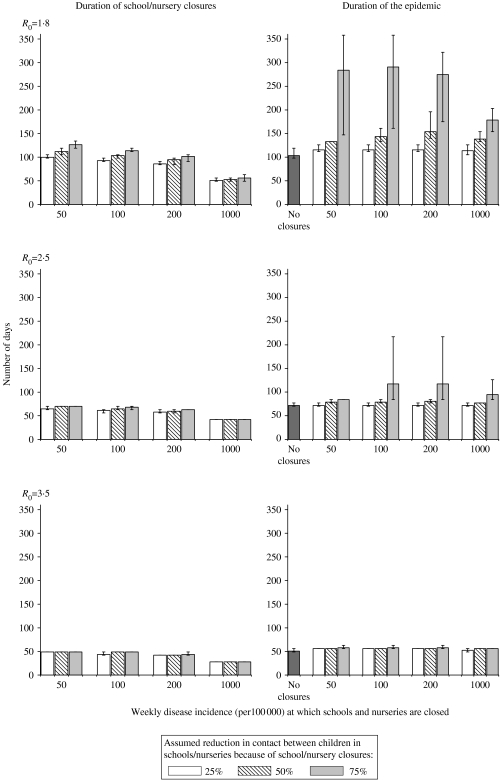
Many countries plan to close schools during a future influenza pandemic, although the potential impact is poorly understood. We apply a model of the transmission dynamics of pandemic influenza to consultation, serological and clinical data from the United Kingdom from the 1957 (Asian) influenza pandemic, to estimate the basic reproduction number (R0), the proportion of infected individuals who experience clinical symptoms and the impact of school/nursery closures. The R0 for Asian influenza was about 1.8 and 60-65% of infected individuals were estimated to have experienced clinical symptoms. During a future pandemic, closure of schools/nurseries could reduce the epidemic size only by a very small amount (<10%) if R0 is high (e.g. 2.5 or 3.5), and modest reductions, e.g. 22% might be possible if it is low (1.8) and schools are closed early, depending on assumptions about contact patterns. Further data on contact patterns and their dependence on school closures are needed.
Figures
References
-
- World Health Organization World Health Organization; 2005. . WHO global influenza preparedness plan. The role of WHO and recommendations for national measures before and during pandemics. ; WHO/CDS/CSR/GIP/2005.5.
-
- Fine PE, Clarkson JA. Measles in England and Wales – I: An analysis of factors underlying seasonal patterns. International Journal of Epidemiology. 1982;11:5–14. - PubMed
-
- Heymann A et al. Influence of school closure on the incidence of viral respiratory diseases among children and on health care utilization. Pediatric Infectious Disease Journal. 2004;23:675–677. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
