

Mutations in ATP-sensitive K+ channel genes cause transient neonatal diabetes and permanent diabetes in childhood or adulthood
- PMID: 17446535
- PMCID: PMC7611811
- DOI: 10.2337/db07-0043
Mutations in ATP-sensitive K+ channel genes cause transient neonatal diabetes and permanent diabetes in childhood or adulthood
Erratum in
- Diabetes. 2008 Feb;57(2):523
Abstract
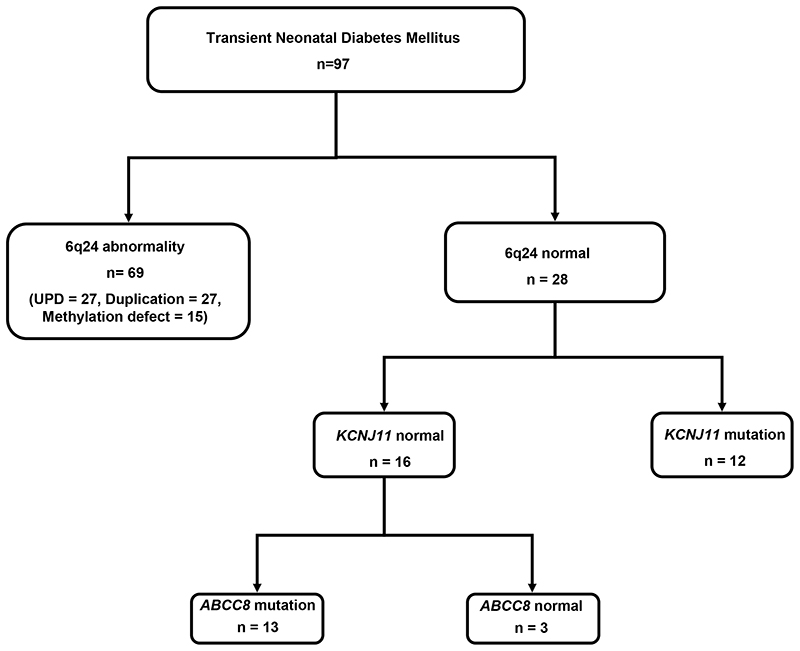
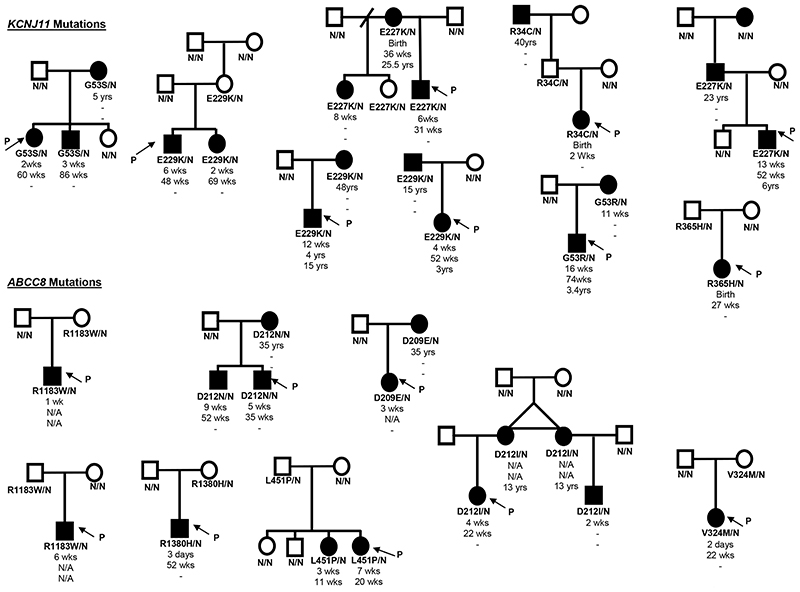
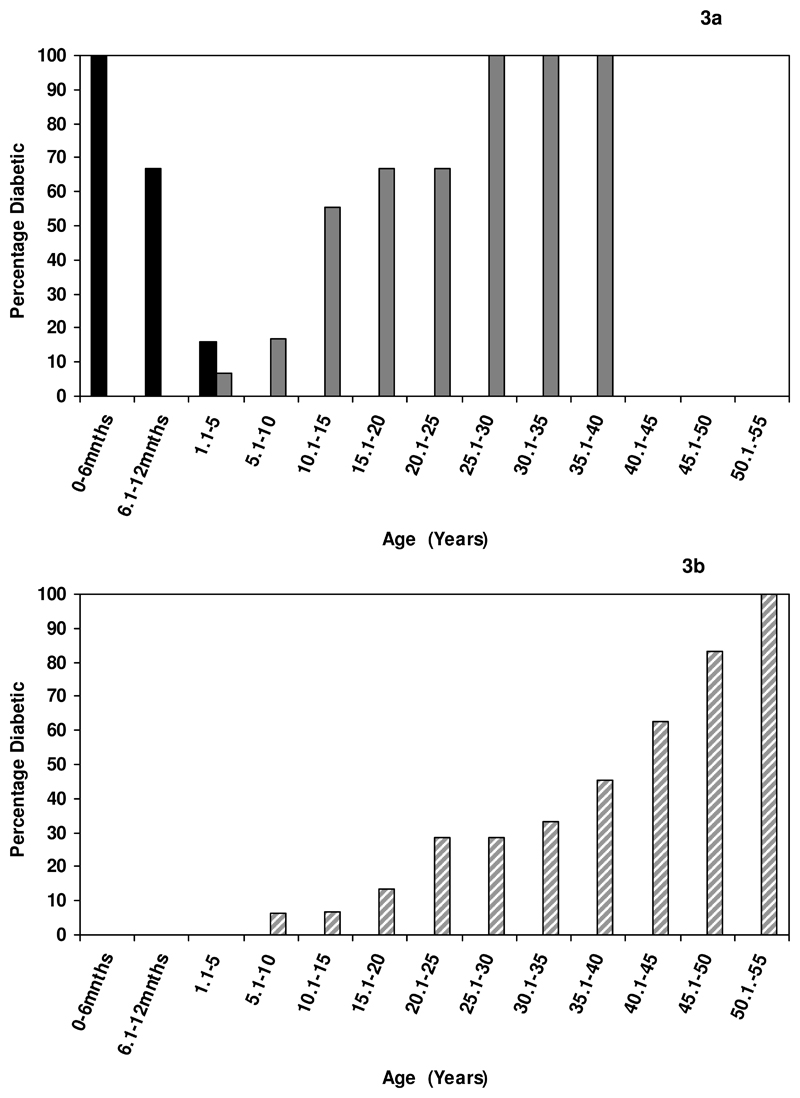
Transient neonatal diabetes mellitus (TNDM) is diagnosed in the first 6 months of life, with remission in infancy or early childhood. For approximately 50% of patients, their diabetes will relapse in later life. The majority of cases result from anomalies of the imprinted region on chromosome 6q24, and 14 patients with ATP-sensitive K+ channel (K(ATP) channel) gene mutations have been reported. We determined the 6q24 status in 97 patients with TNDM. In patients in whom no abnormality was identified, the KCNJ11 gene and/or ABCC8 gene, which encode the Kir6.2 and SUR1 subunits of the pancreatic beta-cell K(ATP) channel, were sequenced. K(ATP) channel mutations were found in 25 of 97 (26%) TNDM probands (12 KCNJ11 and 13 ABCC8), while 69 of 97 (71%) had chromosome 6q24 abnormalities. The phenotype associated with KCNJ11 and ABCC8 mutations was similar but markedly different from 6q24 patients who had a lower birth weight and who were diagnosed and remitted earlier (all P < 0.001). K(ATP) channel mutations were identified in 26 additional family members, 17 of whom had diabetes. Of 42 diabetic patients, 91% diagnosed before 6 months remitted, but those diagnosed after 6 months had permanent diabetes (P < 0.0001). K(ATP) channel mutations account for 89% of patients with non-6q24 TNDM and result in a discrete clinical subtype that includes biphasic diabetes that can be treated with sulfonylureas. Remitting neonatal diabetes was observed in two of three mutation carriers, and permanent diabetes occurred after 6 months of age in subjects without an initial diagnosis of neonatal diabetes.
Figures
References
-
- Temple IK, Gardner RJ, Mackay DJ, Barber JC, Robinson DO, Shield JP. Transient neonatal diabetes: widening the understanding of the etiopathogenesis of diabetes. Diabetes. 2000;49:1359–1366. - PubMed
-
- Temple IK, Gardner RJ, Robinson DO, Kibirige MS, Ferguson AW, Baum JD, Barber JCK, James RS, Shield JPH. Further evidence for an imprinted gene for neonatal diabetes localised to chromosome 6q22-q23. Hum Molec Genet. 1996;5:1117–1124. - PubMed
-
- Gardner RJ, Mackay DJ, Mungall AJ, Polychronakos C, Siebert R, Shield JP, Temple IK, Robinson DO. An imprinted locus associated with transient neonatal diabetes mellitus. Hum Mol Genet. 2000;9:589–596. - PubMed
-
- Gloyn AL, Reimann F, Girard C, Edghill EL, Proks P, Pearson ER, Temple IK, Mackay DJ, Shield JP, Freedenberg D, Noyes K, et al. Relapsing diabetes can result from moderately activating mutations in KCNJ11. Hum Mol Genet. 2005;14:925–934. - PubMed
-
- Yorifuji T, Nagashima K, Kurokawa K, Kawai M, Oishi M, Akazawa Y, Hosokawa M, Yamada Y, Inagaki N, Nakahata T. The C42R mutation in the Kir6.2 (KCNJ11) gene as a cause of transient neonatal diabetes, childhood diabetes, or later-onset, apparently type 2 diabetes mellitus. J Clin Endocrinol Metab. 2005;90:3174–3178. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
