

Implementing routine cognitive screening of older adults in primary care: process and impact on physician behavior
- PMID: 17447100
- PMCID: PMC2219855
- DOI: 10.1007/s11606-007-0202-8
Implementing routine cognitive screening of older adults in primary care: process and impact on physician behavior
Erratum in
- J Gen Intern Med. 2007 Aug;22(8):1224
Abstract
Background: Early detection of cognitive impairment is a goal of high-quality geriatric medical care, but new approaches are needed to reduce rates of missed cases.
Objective: To evaluate whether adding routine cognitive screening to primary care visits for older adults increases rates of dementia diagnosis, specialist referral, or prescribing of antidementia medications.
Setting: Four primary care clinics in a university-affiliated primary care network.
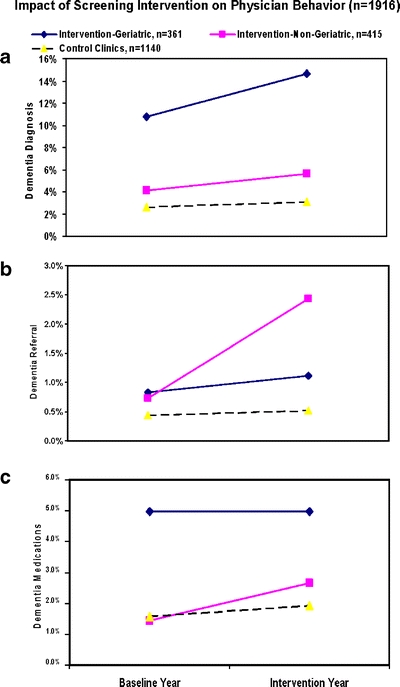
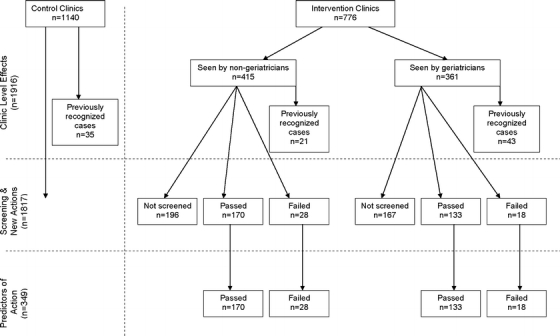
Design: A quality improvement screening project and quasiexperimental comparison of 2 intervention clinics and 2 control clinics. The Mini-Cog was administered by medical assistants to intervention clinic patients aged 65+ years. Rates of dementia diagnoses, referrals, and medication prescribing were tracked over time using computerized administrative data.
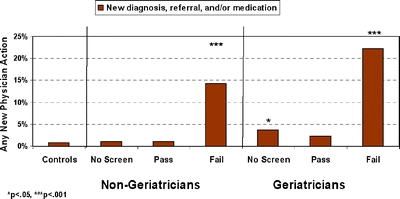
Results: Twenty-six medical assistants successfully screened 70% (n = 524) of all eligible patients who made at least 1 clinic visit during the intervention period; 18% screened positive. There were no complaints about workflow interruption. Relative to baseline rates and control clinics, Mini-Cog screening was associated with increased dementia diagnoses, specialist referrals, and prescribing of cognitive enhancing medications. Patients without previous dementia indicators who had a positive Mini-Cog were more likely than all other patients to receive a new dementia diagnosis, specialty referral, or cognitive enhancing medication. However, relevant physician action occurred in only 17% of screen-positive patients. Responses were most related to the lowest Mini-Cog score level (0/5) and advanced age.
Conclusion: Mini-Cog screening by office staff is feasible in primary care practice and has measurable effects on physician behavior. However, new physician action relevant to dementia was likely to occur only when impairment was severe, and additional efforts are needed to help primary care physicians follow up appropriately on information suggesting cognitive impairment in older patients.
Figures
References
-
- Callahan CM, Hendrie HC, Tierney WM. Documentation and evaluation of cognitive impairment in elderly primary care patients. Ann Intern Med. 1995;122:422–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
