

Cytokine profiles as markers of disease severity in sepsis: a multiplex analysis
- PMID: 17448250
- PMCID: PMC2206478
- DOI: 10.1186/cc5783
Cytokine profiles as markers of disease severity in sepsis: a multiplex analysis
Abstract
Introduction: The current shortage of accurate and readily available, validated biomarkers of disease severity in sepsis is an important limitation when attempting to stratify patients into homogeneous groups, in order to study pathogenesis or develop therapeutic interventions. The aim of the present study was to determine the cytokine profile in plasma of patients with severe sepsis by using a multiplex system for simultaneous detection of 17 cytokines.
Methods: This was a prospective cohort study conducted in four tertiary hospitals. A total of 60 patients with a recent diagnosis of severe sepsis were included. Plasma samples were collected for measurement of cytokine concentrations. A multiplex analysis was performed to evaluate levels of 17 cytokines (IL-1 beta, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12, IL-13, IL-17, interferon-gamma, granulocyte colony-stimulating factor [G-CSF], granulocyte-macrophage colony-stimulating factor, monocyte chemoattractant protein [MCP]-1, macrophage inflammatory protein-1 and tumour necrosis factor-alpha). Cytokine concentrations were related to the presence of severe sepsis or septic shock, the severity and evolution of organ failure, and early and late mortality.
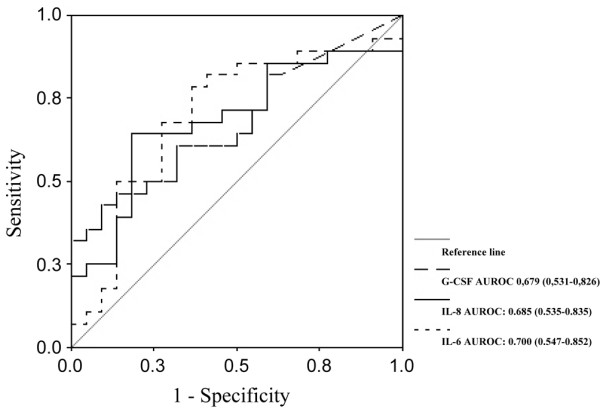
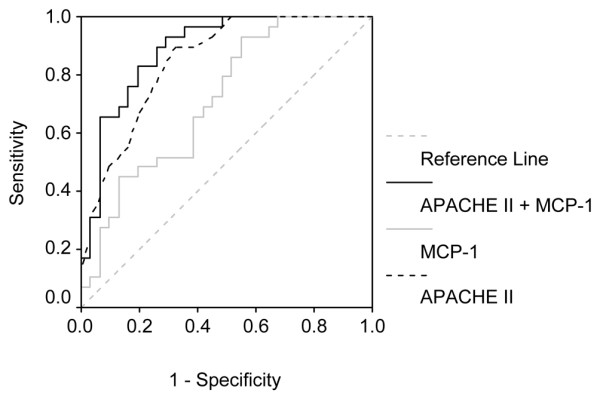
Results: Concentrations of IL-1 beta, IL-6, IL-7, IL-8, IL-10, IL-13, interferon-gamma, MCP-1 and tumour necrosis factor-alpha were significantly higher in septic shock patients than in those with severe sepsis. Cytokine concentrations were associated with severity and evolution of organ dysfunction. With regard to the severity of organ dysfunction on day 1, IL-8 and MCP-1 exhibited the best correlation with Sequential Organ Failure Assessment score. In addition, IL-6, IL-8 and G-CSF concentrations during the first 24 hours were predictive of worsening organ dysfunction or failure of organ dysfunction to improve on day three. In terms of predicting mortality, the cytokines IL-1 beta, IL-4, IL-6, IL-8, MCP-1 and G-CSF had good accuracy for predicting early mortality (< 48 hours), and IL-8 and MCP-1 had the best accuracy for predicting mortality at 28 days. In multivariate analysis, only MCP-1 was independently associated with prognosis.
Conclusion: In this exploratory analysis we demonstrated that use of a multiple cytokine assay platform allowed identification of distinct cytokine profiles associated with sepsis severity, evolution of organ failure and death.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
