

Abnormal left ventricular longitudinal functional reserve in patients with diabetes mellitus: implication for detecting subclinical myocardial dysfunction using exercise tissue Doppler echocardiography
- PMID: 17449503
- PMCID: PMC2095774
- DOI: 10.1136/hrt.2006.101667
Abnormal left ventricular longitudinal functional reserve in patients with diabetes mellitus: implication for detecting subclinical myocardial dysfunction using exercise tissue Doppler echocardiography
Abstract
Background: Subclinical myocardial dysfunction occurs in a significant number of patients with type 2 diabetes. Assessment of ventricular long-axis function by measuring mitral annular velocities using tissue Doppler echocardiography (TDE) is thought to provide a more sensitive index of systolic and diastolic function. We hypothesised that augmentation of left ventricular (LV) longitudinal contraction and relaxation during exercise would be blunted in patients with type 2 diabetes.
Methods: Mitral annular systolic (S') and early diastolic (E') velocities were measured at rest and during supine bicycle exercise (25 W, 3 min increments) in 53 patients (27 male, mean age 53+/-14 years) with type 2 diabetes and 53 subjects with age and gender-matched control. None had echocardiographic evidence of resting or inducible myocardial ischaemia.
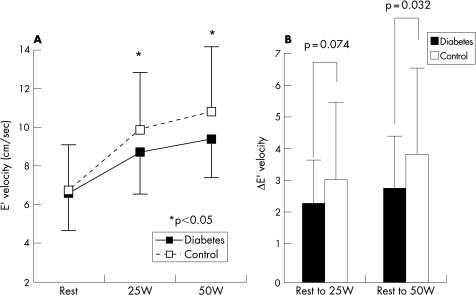
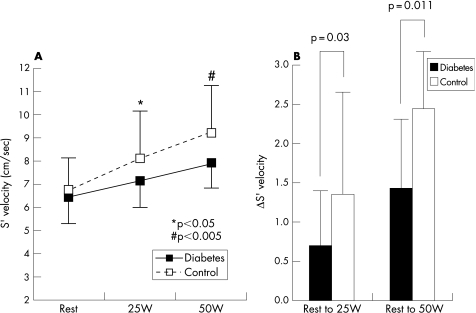
Results: There were no significant differences in mitral inflow velocities at rest between the two groups. E' and S' at rest were also similar between the groups. However, S' (7.1+/-1.3 vs 8.3+/-1.8 cm/s at 25 W, p = 0.0021; 8.1+/-1.5 vs 9.1+/-2.0 cm/s at 50 W, p = 0.026) and E' (8.5+/-2.3 vs 9.9+/-3.1 cm/s at 25 W, p = 0.054; 9.1+/-2.1 vs 10.9+/-2.5 cm/s at 50 W, p = 0.0093) during exercise were significantly lower in patients with diabetes compared with controls. Longitudinal systolic and diastolic function reserve indices were significantly lower in patients with diabetes compared with that of controls (systolic index, 0.6+/-0.70 vs 1.2+/-1.5 cm/s at 25 W, p = 0.029; 1.2+/-1.2 vs 2.1+/-1.6 cm/s at 50 W, p = 0.009; diastolic index, 1.9+/-1.2 vs 2.5+/-2.2 cm/s at 25 W, p = 0.07; 2.3+/-1.3 vs 3.2+/-2.2 cm/s at 50 W, p = 0.031).
Conclusion: In conclusion, unlike resting mitral inflow and annular velocities, changes of systolic and diastolic velocities of the mitral annulus during exercise were significantly reduced in patients with type 2 diabetes compared with the control group. The assessment of LV longitudinal functional reserve with exercise using TDE appears to be helpful in identifying early myocardial dysfunction in patients with type 2 diabetes.
Conflict of interest statement
Competing interests: None.
Comment in
-
Exercise echocardiography.Heart. 2009 Jan;95(1):83. Heart. 2009. PMID: 19047445 No abstract available.
References
-
- Tang W H, Young J B. Cardiomyopathy and heart failure in diabetes. Endocrinol Metab Clin North Am 2001301031–1046. - PubMed
-
- Fang Z Y, Yuda S, Anderson V.et al Echocardiographic detection of early diabetic myocardial disease. J Am Coll Cardiol 200341611–617. - PubMed
-
- Struthers A D, Morris A D. Screening for and treating left‐ventricular abnormalities in diabetes mellitus: a new way of reducing cardiac deaths. Lancet 20023591430–1432. - PubMed
-
- Fang Z Y, Schull‐Meade R, Leano R.et al Screening for heart disease in diabetic subjects. Am Heart J 2005149349–354. - PubMed
-
- Marwick T H. Tissue Doppler imaging for evaluation of myocardial function in patients with diabetes mellitus. Curr Opin Cardiol 200419442–446. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical