

Risk factors for prostate cancer incidence and progression in the health professionals follow-up study
- PMID: 17450530
- PMCID: PMC2430098
- DOI: 10.1002/ijc.22788
Risk factors for prostate cancer incidence and progression in the health professionals follow-up study
Abstract
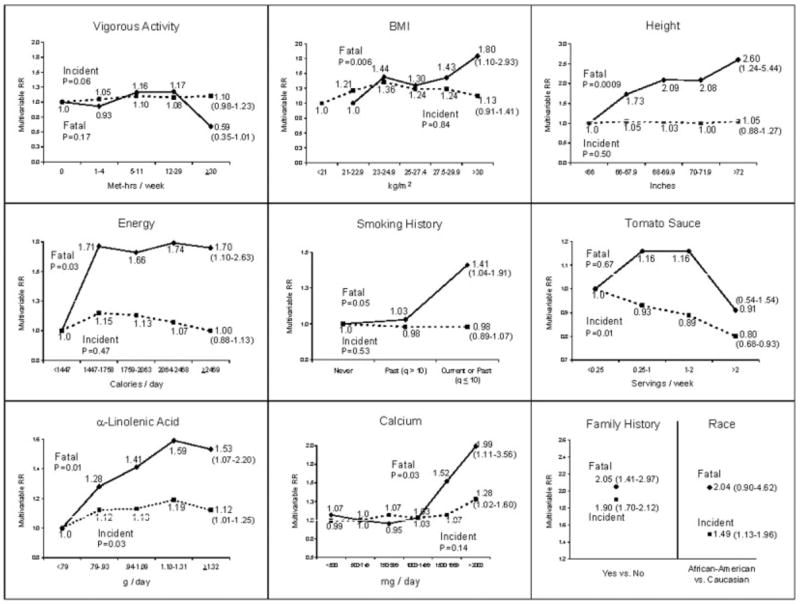
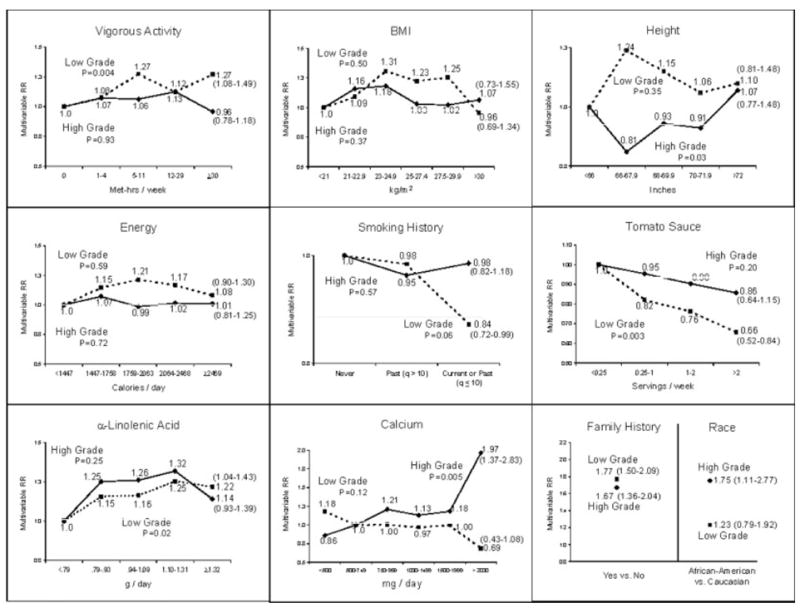
Risk factors for prostate cancer could differ for various sub-groups, such as for "aggressive" and "non-aggressive" cancers or by grade or stage. Determinants of mortality could differ from those for incidence. Using data from the Health Professionals Follow-Up Study, we re-examined 10 factors (cigarette smoking history, physical activity, BMI, family history of prostate cancer, race, height, total energy consumption, and intakes of calcium, tomato sauce and alpha-linolenic acid) using multivariable Cox regression in relation to multiple subcategories for prostate cancer risk. These were factors that we previously found to be predictors of prostate cancer incidence or advanced prostate cancer in this cohort, and that have some support in the literature. In this analysis, only 4 factors had a clear statistically significant association with overall incident prostate cancer: African-American race, positive family history, higher tomato sauce intake (inversely) and alpha-linolenic acid intake. In contrast, for fatal prostate cancer, recent smoking history, taller height, higher BMI, family history, and high intakes of total energy, calcium and alpha-linolenic acid were associated with a statistically significant increased risk. Higher vigorous physical activity level was associated with lower risk. In relation to these risk factors, advanced stage at diagnosis was a good surrogate for fatal prostate cancer, but high-grade (Gleason >/= 7 or Gleason >/= 8) was not. Only for high calcium intake was there a close correspondence for associations among high-grade cancer, advanced and fatal prostate cancer. Tomato sauce (inversely) and alpha-linolenic acid (positively) intakes were strong predictors of advanced cancer among those with low-grade cancers at diagnosis. Although the proportion of advanced stage cancers was much lower after PSA screening began, risk factors for advanced stage prostate cancers were similar in the pre-PSA and PSA era. The complexity of the clinical and pathologic manifestations of prostate cancer must be considered in the design and interpretation of studies.
Figures
References
-
- Parkin DM, Whelan SL, Ferlay J, Teppo L, Thomas D. Cancer incidence in five continents, International agency for research on cancer. Vol. 155. Lyon: IARC Scientific Publications; 2003.
-
- Parkin DM, Muir CS, Whelan SL, Gao YT, Ferlay J, Powell J. Cancer incidence in five continents, International agency for research on cancer. Lyon, France: IARC Scientific Publications; 1992.
-
- Haenszel W, Kurihara M. Studies of Japanese migrants. I Mortality from cancer and other diseases among Japanese in the United States. J Natl Cancer Inst. 1968;40:43–68. - PubMed
-
- Yu H, Harris RE, Gao YT, Gao R, Wynder EL. Comparative epidemiology of cancers of the colon, rectum, prostate and breast in Shanghai, China versus the United States. Int J Epidemiol. 1991;20:76–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
