

Case mix, outcome and activity for patients admitted to intensive care units requiring chronic renal dialysis: a secondary analysis of the ICNARC Case Mix Programme Database
- PMID: 17451605
- PMCID: PMC2206479
- DOI: 10.1186/cc5785
Case mix, outcome and activity for patients admitted to intensive care units requiring chronic renal dialysis: a secondary analysis of the ICNARC Case Mix Programme Database
Abstract
Introduction: This report describes the case mix, outcome and activity for admissions to intensive care units (ICUs) of patients who require prior chronic renal dialysis for end-stage renal failure (ESRF), and investigates the effect of case mix factors on outcome.
Methods: This was a secondary analysis of a high-quality clinical database, namely the Intensive Care National Audit & Research Centre (ICNARC) Case Mix Programme Database, which includes 276,731 admissions to 170 adult ICUs across England, Wales and Northern Ireland from 1995 to 2004.
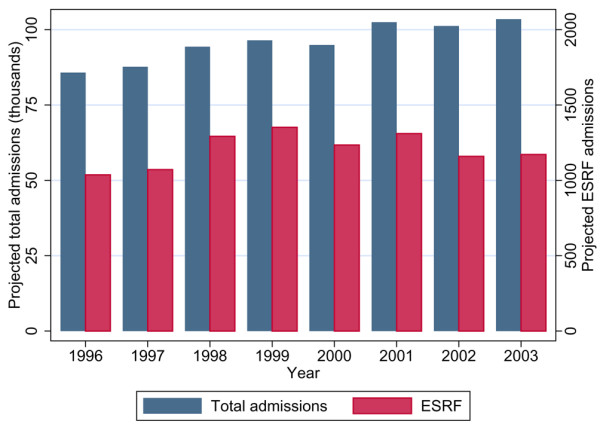
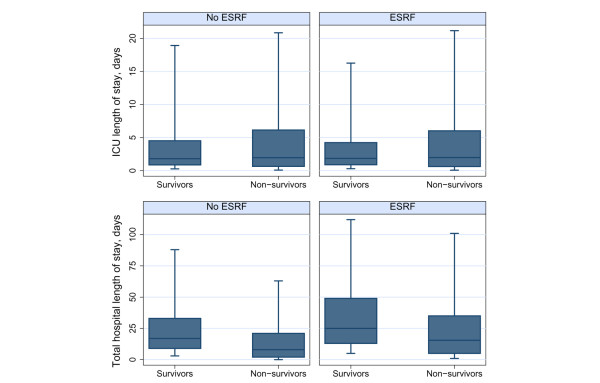
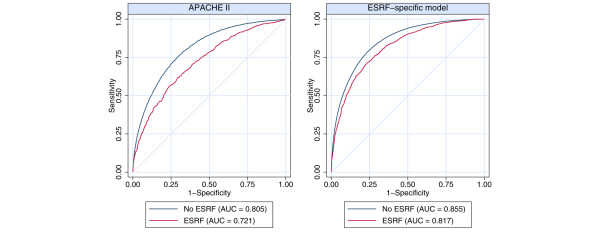
Results: During the eight year study period, 1.3% (n = 3,420) of all patients admitted to ICU were receiving chronic renal dialysis before ICU admission. This represents an estimated ICU utilization of six admissions (32 bed-days) per 100 dialysis patient-years. The ESRF group was younger (mean age 57.3 years versus 59.5 years) and more likely to be male (60.2% versus 57.9%) than those without ESRF. Acute Physiology and Chronic Health Evaluation II score and Acute Physiology Score revealed greater severity of illness on admission in patients with ESRF (mean 24.7 versus 16.6 and 17.2 versus 12.6, respectively). Length of stay in ICU was comparable between groups (median 1.9 days versus 1.8 days) and ICU mortality was only slightly elevated in the ESRF group (26.3% versus 20.8%). However, the ESRF group had protracted overall hospital stay (median 25 days versus 17 days), and increased hospital mortality (45.3% versus 31.2%) and ICU readmission (9.0% vs. 4.7%). Multiple logistic regression analysis adjusted for case mix identified the increased hospital mortality to be associated with increasing age, emergency surgery and nonsurgical cases, cardiopulmonary resuscitation before ICU admission and extremes of physiological norms. The adjusted odds ratio for ultimate hospital mortality associated with chronic renal dialysis was 1.24 (95% confidence interval 1.13 to 1.37).
Conclusion: Patients with ESRF admitted to UK ICUs are more likely to be male and younger, with a medical cause of admission, and to have greater severity of illness than the non-ESRF population. Outcomes on the ICU were comparable between the two groups, but those patients with ESRF had greater readmission rates, prolonged post-ICU hospital stay and increased post-ICU hospital mortality. This study is by far the largest comparative outcome analysis to date in patients with ESRF admitted to the ICU. It may help to inform clinical decision-making and resource requirements for this patient population.
Figures
Comment in
-
Haemodialysis and peritoneal dialysis patients admitted to intensive care units.Crit Care. 2007;11(3):133. doi: 10.1186/cc5914. Crit Care. 2007. PMID: 17561985 Free PMC article.
References
-
- Schetz M. Renal replacement therapy in patients with chronic (end stage) renal failure and acute illness. In: Ronco C, Bellomo R, editor. Critical Care Nephrology. Boston, MA: Kluwer Academic Publishers; 1998. pp. 1139–1153.
-
- Dara SI, Afessa B, Bajwa AA, Albright RC. Outcome of patients with end-stage renal disease admitted to the intensive care unit. Mayo Clin Proc. 2004;79:1385–1390. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
