

Modeling hepatitis C virus dynamics: liver regeneration and critical drug efficacy
- PMID: 17451750
- PMCID: PMC2265666
- DOI: 10.1016/j.jtbi.2007.03.006
Modeling hepatitis C virus dynamics: liver regeneration and critical drug efficacy
Abstract
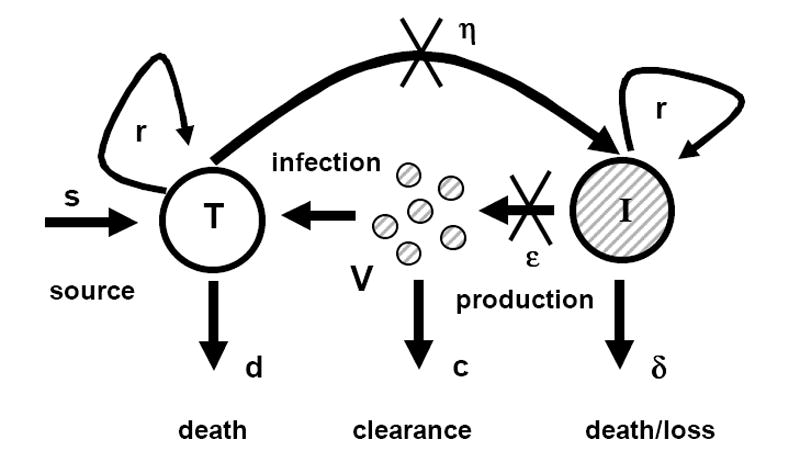
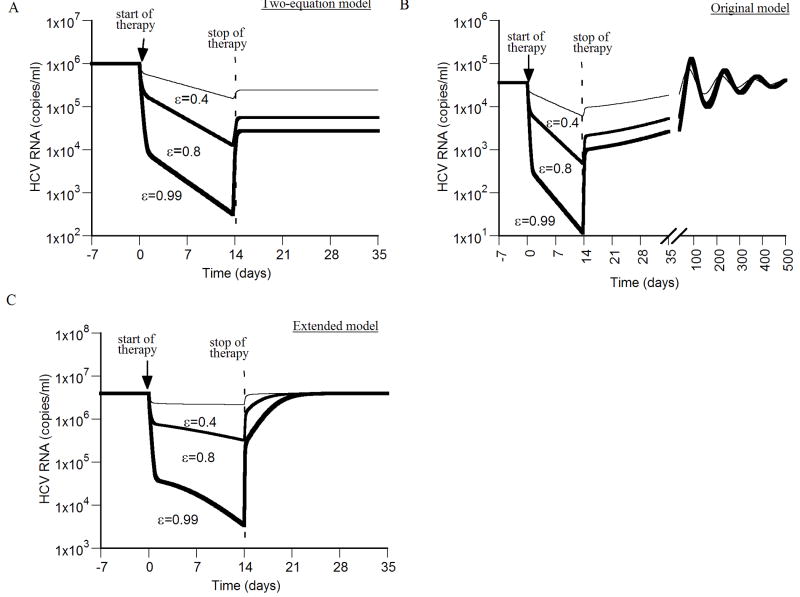
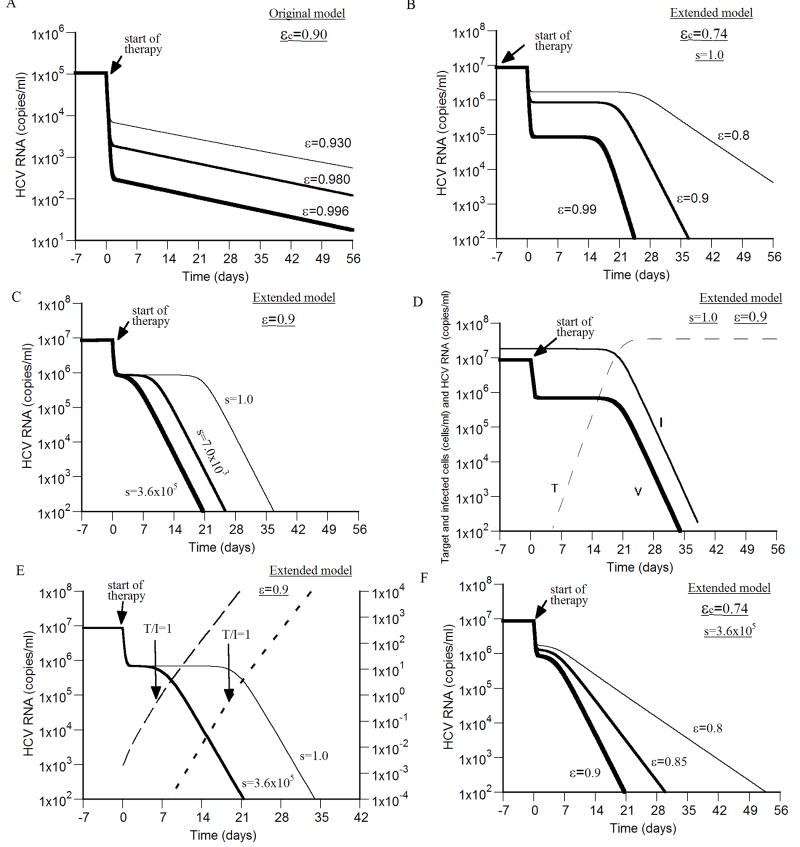
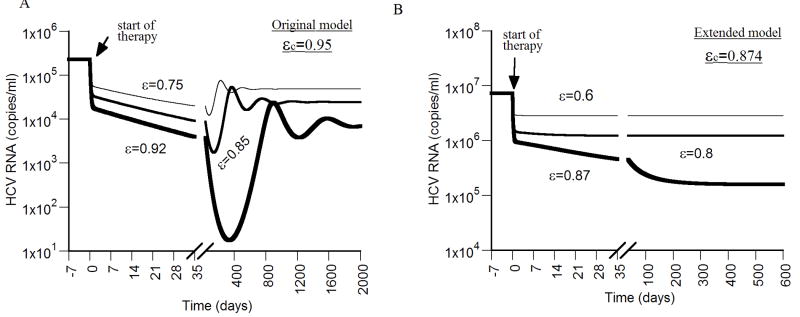
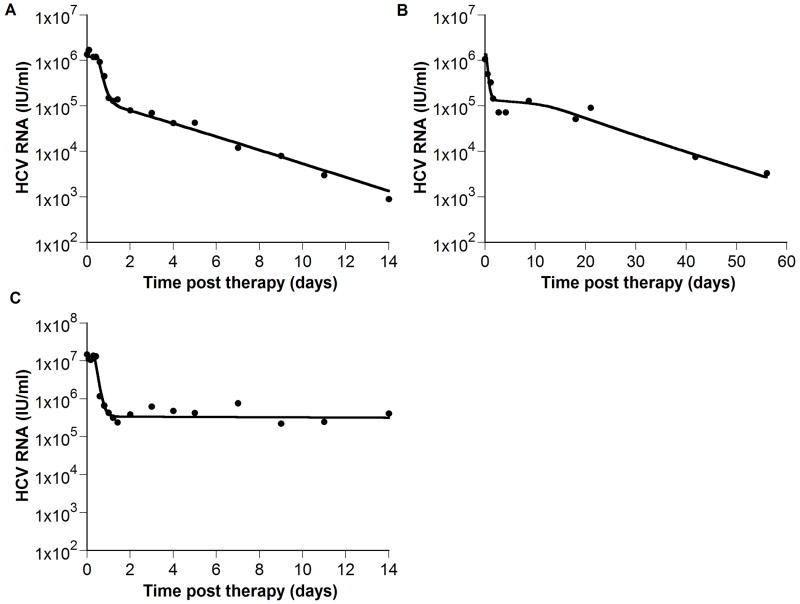
Mathematical models for hepatitis C viral (HCV) RNA kinetics have provided a means of evaluating the antiviral effectiveness of therapy, of estimating parameters such as the rate of HCV RNA clearance, and they have suggested mechanism of action against HCV for both interferon and ribavirin. Nevertheless, the model that was originally formulated by Neumann et al. [1998. Hepatitis C viral dynamics in vivo and the antiviral efficacy of interferon-alpha therapy. Science 282 (5386), 103-107] is unable to explain all of the observed HCV RNA profiles under treatment e.g., a triphasic viral decay and a viral rebound to baseline values after the cessation of therapy. Further, the half-life of productively HCV-infected cells, estimated from the second phase HCV RNA decline slope, is very variable and sometimes zero with no clear understanding of why. We show that extending the original model by including hepatocyte proliferation yields a more realistic model without any of these deficiencies. Further, we define and characterize a critical drug efficacy, such that for efficacies above the critical value HCV is ultimately cleared, while for efficacies below it, a new chronically infected viral steady-state level is reached.
Figures
Similar articles
-
Modeling the dynamics of hepatitis C virus with combined antiviral drug therapy: interferon and ribavirin.Math Biosci. 2013 Oct;245(2):235-48. doi: 10.1016/j.mbs.2013.07.005. Epub 2013 Jul 25. Math Biosci. 2013. PMID: 23891586
-
Mathematical modeling of HCV infection and treatment.Methods Mol Biol. 2009;510:439-53. doi: 10.1007/978-1-59745-394-3_33. Methods Mol Biol. 2009. PMID: 19009281
-
New kinetic models for the hepatitis C virus.Hepatology. 2005 Oct;42(4):749-54. doi: 10.1002/hep.20882. Hepatology. 2005. PMID: 16175615 Review.
-
Hepatitis C virus kinetics.Antivir Ther. 2000 Jun;5(2):85-90. Antivir Ther. 2000. PMID: 10971860 Review.
-
Clinical implications of hepatitis C viral kinetics.J Hepatol. 1999;31 Suppl 1:61-4. doi: 10.1016/s0168-8278(99)80376-6. J Hepatol. 1999. PMID: 10622562 Review.
Cited by
-
Hepatitis C virus RNA kinetics: drug efficacy and the rate of HCV-infected cells loss.World J Gastroenterol. 2007 Jun 7;13(21):3020-1. doi: 10.3748/wjg.v13.i21.3020. World J Gastroenterol. 2007. PMID: 17589958 Free PMC article. No abstract available.
-
Mathematical modeling of within-host Zika virus dynamics.Immunol Rev. 2018 Sep;285(1):81-96. doi: 10.1111/imr.12687. Immunol Rev. 2018. PMID: 30129207 Free PMC article. Review.
-
Modeling population heterogeneity in viral dynamics for chronic hepatitis C infection: Insights from Phase 3 telaprevir clinical studies.J Pharmacokinet Pharmacodyn. 2015 Dec;42(6):681-98. doi: 10.1007/s10928-015-9435-z. Epub 2015 Aug 20. J Pharmacokinet Pharmacodyn. 2015. PMID: 26289844
-
Mechanistic Modeling of SARS-CoV-2 and Other Infectious Diseases and the Effects of Therapeutics.Clin Pharmacol Ther. 2021 Apr;109(4):829-840. doi: 10.1002/cpt.2160. Epub 2021 Mar 8. Clin Pharmacol Ther. 2021. PMID: 33410134 Free PMC article. Review.
-
Modeling challenges of hepatitis D virus kinetics during bulevirtide-based therapy.JHEP Rep. 2024 Sep 6;7(2):101211. doi: 10.1016/j.jhepr.2024.101211. eCollection 2025 Feb. JHEP Rep. 2024. PMID: 39867682 Free PMC article. No abstract available.
References
-
- Alter MJ, Margolis HS, Krawczynski K, Judson FN, Mares A, Alexander WJ, Hu PY, Miller JK, Gerber MA, Sampliner RE. The natural history of community-acquired hepatitis C in the United States. The Sentinel Counties Chronic non-A, non-B Hepatitis Study Team. N Engl J Med. 1992;327(27):1899–1905. - PubMed
-
- Callaway DS, Perelson AS. HIV-1 infection and low steady state viral loads. Bull Math Biol. 2002;64(1):29–64. - PubMed
-
- Colombatto P, Civitano L, Oliveri F, Coco B, Ciccorossi P, Flichman D, Campa M, Bonino F, Brunetto MR. Sustained response to interferon-ribavirin combination therapy predicted by a model of hepatitis C virus dynamics using both HCV RNA and alanine aminotransferase. Antivir Ther. 2003;8(6):519–530. - PubMed
-
- Dahari H, Feliu A, Garcia-Retortillo M, Forns X, Neumann AU. Second hepatitis C replication compartment indicated by viral dynamics during liver transplantation. J Hepatol. 2005a;42(4):491–498. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
