

Long-term survival after successful inhospital cardiac arrest resuscitation
- PMID: 17452161
- PMCID: PMC3156467
- DOI: 10.1016/j.ahj.2007.02.011
Long-term survival after successful inhospital cardiac arrest resuscitation
Abstract
Background: Little is known about long-term outcomes of patients who survive inhospital cardiac arrest.
Methods: We examined long-term survival after inhospital cardiac arrest and whether procedural changes that improved survival to discharge impacted long-term survival. Consecutive inhospital arrests in the Atlanta Veterans Affairs Medical Center (Atlanta, GA) from 1995 to 2004 (n = 732) were retrospectively analyzed. Data regarding the arrest was obtained, including age, left ventricular ejection fraction, medications, and comorbidities, presenting rhythm, location of arrest, code duration, and outcomes. Long-term mortality data was obtained based on chart and Social Security Death Index reviews. Further data was gathered on internal cardioverter-defibrillator presence and use in survivors.
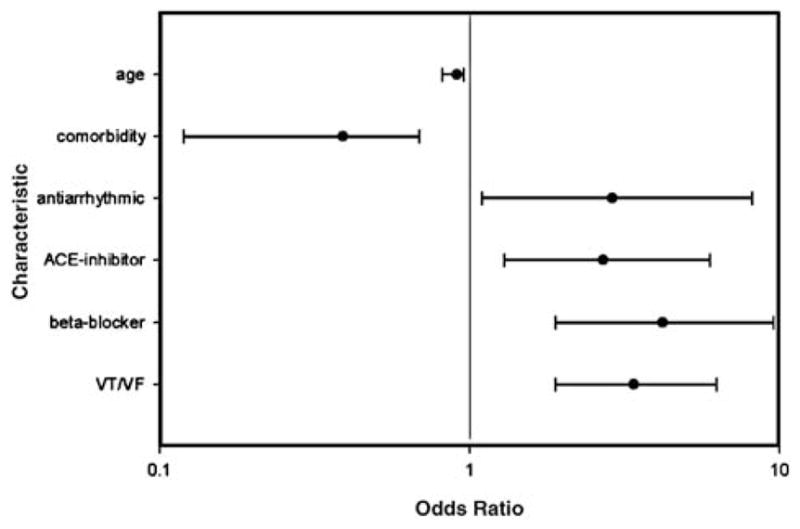
Results: Overall, 49 subjects (6.6%) survived to discharge. Univariate analysis found that ventricular tachycardia/ventricular fibrillation and the use of beta-blockers, angiotensin-converting enzyme inhibitors, and antiarrhythmics at the time of arrest were associated with increased survival, whereas advancing age and comorbidities were associated with a higher risk of mortality. Multivariate analysis determined that age, rhythm, and comorbidities independently affected survival. Implementation of a resuscitation program previously documented to improve survival to discharge did not translate to durable long-term survival. Three-year survival rate after discharge was only 41%. Alternatively, subjects with internal cardioverter-defibrillator showed a 36% improvement in 3-year survival rate to 77% (P = .001).
Conclusions: Subjects with inhospital cardiac arrest have poor long-term prognoses. A strategy that improved inhospital survival did not alter long-term mortality rate. Thus, survival to discharge may not be a sufficient end point for future resuscitation trials.
Figures


References
-
- Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed-chest cardiac massage. JAMA. 1960;173:1064–7. - PubMed
-
- Ballew KA, Philbrick JT. Causes of variation in reported in-hospital CPR survival: a critical review. Resuscitation. 1995;30:203–15.
-
- White RD, Hankins DG, Atkinson EJ. Patient outcomes following defibrillation with a low energy biphasic truncated exponential waveform in out-of-hospital cardiac arrest. Resuscitation. 2001;49:9–14. - PubMed
-
- White RD. Technologic advances and program initiatives in public access defibrillation using automated external defibrillators. Curr Opin Crit Care. 2001;7:145–51. - PubMed
-
- Ruskin JN, DiMarco JP, Garan H. Out-of-hospital cardiac arrest: electrophysiologic observations and selection of long-term anti-arrhythmic therapy. N Engl J Med. 1980;303:607–13. - PubMed
