

Phase II study of metronomic chemotherapy for recurrent malignant gliomas in adults
- PMID: 17452651
- PMCID: PMC1907419
- DOI: 10.1215/15228517-2007-006
Phase II study of metronomic chemotherapy for recurrent malignant gliomas in adults
Abstract
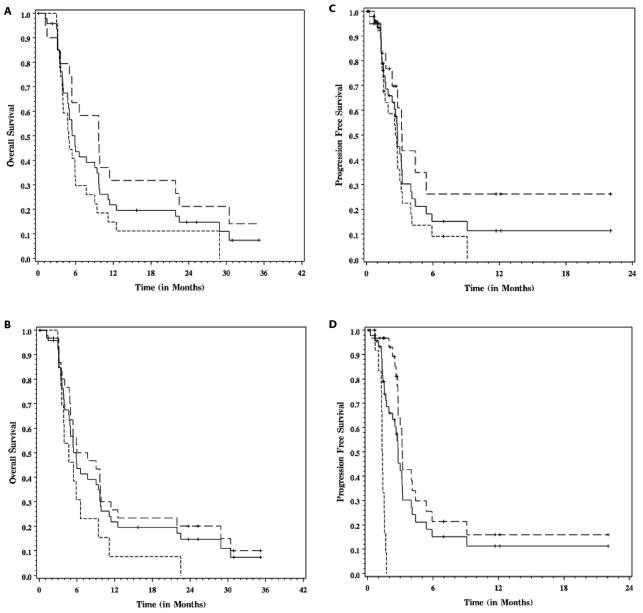
Preclinical evidence suggests that continuous low-dose daily (metronomic) chemotherapy may inhibit tumor endothelial cell proliferation (angiogenesis) and prevent tumor growth. This phase II study evaluated the feasibility of this antiangiogenic chemotherapy regimen in adults with recurrent malignant gliomas. The regimen consisted of low-dose etoposide (35 mg/m2 [maximum, 100 mg/day] daily for 21 days), alternating every 21 days with cyclophosphamide (2 mg/kg [maximum, 100 mg/day] daily for 21 days), in combination with daily thalidomide and celecoxib, in adult patients with recurrent malignant gliomas. Serum and urine samples were collected for measurement of angiogenic peptides. Forty-eight patients were enrolled (15 female, 33 male). Twenty-eight patients had glioblastoma multiforme (GBMs), and 20 had anaplastic gliomas (AGs). Median age was 53 years (range, 33-74 years), and median KPS was 70 (range, 60-100). Therapy was reasonably well tolerated in this heavily pretreated population. Two percent of patients had partial response, 9% had a minor response, 59% had stable disease, and 30% had progressive disease. For GBM patients, median progression-free survival (PFS) was 11 weeks, six-month PFS (6M-PFS) was 9%, and median overall survival (OS) was 21 weeks. For AG patients, median PFS was 14 weeks, 6M-PFS was 26%, and median OS was 41.5 weeks. In a limited subset of patients, serum and urine angiogenic peptides did not correlate with response or survival (p > 0.05). Although there were some responders, this four-drug, oral metronomic regimen did not significantly improve OS in this heavily pretreated group of patients who were generally not eligible for conventional protocols. While metronomic chemotherapy may not be useful in patients with advanced disease, further studies using metronomic chemotherapy combined with more potent antiangiogenic agents in patients with less advanced disease may be warranted.
Figures

References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–996. - PubMed
-
- Brem S, Tsanaclis AM, Gately S, Gross JL, Herblin WF. Immunolocalization of basic fibroblast growth factor to the microvasculature of human brain tumors. Cancer. 1992;70:2673–2680. - PubMed
-
- Kesari S, Ramakrishna N, Sauvageot C, Stiles CD, Wen PY. Targeted molecular therapy of malignant gliomas. Curr Neurol Neurosci Rep. 2005;5:186–197. - PubMed
-
- Plate KH, Breier G, Weich HA, Risau W. Vascular endothelial growth factor is a potential tumour angiogenesis factor in human gliomas in vivo. Nature. 1992;359:845–848. - PubMed
-
- Plate KH, Risau W. Angiogenesis in malignant gliomas. Glia. 1995;15:339–347. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
